As for any other group, education is critical to expanding the life prospects of people with disabilities. In addition, the socialization of children with disabilities (CWD) through education assumes an unusually important role in societies such as India where social exclusion of PWD is significant. Despite its importance, educational outcomes for children and adults with disabilities remain very poor. Illiteracy rates both for all PWD and for school-age disabled children remain much higher than the general population, and school attendance among school age CWD massively lags that of non-disabled children. This chapter discusses first the policy developments in India and internationally on education of CWD. It then presents an educational profile of CWD and PWD, and finds that India’s MDG goals in education will not be met with current performance with respect to children with disabilities. A review of the current performance of public initiatives in the general education system to get CWD into school and improve their learning outcomes follows. An overview of non-government initiatives in PWD education then follows, before conclusions and recommendations.
As in other areas of service delivery, many of the issues discussed in the chapter reflect broader challenges in an education system which is grappling with issues of quality and drop out for children without specific needs even at the primary level. Many of the issues discussed with respect to CWD are thus more acute manifestations of broader challenges. The chapter seeks to identify key constraints on improving participation and learning outcomes for CWD, but equally acknowledges that the agenda is a medium term – in some cases long term – one, which requires prioritization and sequencing in the face of limited institutional capacity, and often constrained resources. Equally, it raises difficult trade-offs for those responsible for allocation of public resources for education. While Indian law and policy are clear in the commitment to the right of all children to basic education, in practice difficult issues arise. For example, if a given fiscal allocation aims to maximize enrollment, minimize drop-out and improve quality of education for all children, there may be tough choices in cases where the resource requirements for CWD are higher than for other children and bringing CWD into the system implies that greater numbers of non-disabled children do not enroll or drop out as a result. This is an area where a rights-based approach and that of economists and utilitarians can conflict.
However, they need not. International evidence suggests that the educational outcomes of non-disabled students can also be improved by inclusion of CWD in integrated classes. While more evidence from developing countries is needed, evidence from Canada and the USA at both pre-school and basic education levels found improved outcomes for non-disabled students from integrated learning. 2 Studies in India on the issue are to date lacking, but evidence from a pre-school study in the slums of Mumbai found that a range of developmental indicators for non-disabled children also improved significantly following the inclusion of disabled children.
Indian and International Policy Developments on Education of CWD
The education of children with disabilities and special needs in India was initiated in the late 1800s, with the establishment of special schools for the Deaf in Bombay in 1883, and for the Blind in Amritsar in 1887. By 1900 numerous special schools for the visually and hearing impaired children were set up across the country. This initiated the tradition of special schools in the country and till the 1970s, this was the dominant mode of service delivery for children with special needs (CSN). 4 It was only in 1974 that the scheme on Integrated Education of Disabled Children (IEDC) broke new ground by stressing the need for educating children with mild to moderate disabilities in regular school settings. However, the tensions between the role of special and general schools for CSN continues today, even after the widespread recognition that inclusion is seen as a more effective educational and social strategy in most cases.
The National Policy on Education (1986) brought the fundamental issue of equality for CSN to the forefront. 5 It stated that the “objective should be to integrate physically and mentally disabled people with the general community as equal partners, to prepare them for normal growth and to enable them to face life with courage and confidence”. While the NPE helped set the stage for further integration and inclusion, only in 1990 did the government provide teeth to the policy through the adoption of the Plan of Action (POA). The POA ambitiously committed to universal enrolment by 2000 for both children with and without disabilities. It also strengthened the NPE by demanding that CSN be educated only in regularly schools and not in special schools as had been allowed earlier. The placement principle for CSN in effect relegated special schools to the status of bridge schools. Children in these schools were expected to obtain training in non-curriculum areas, to help them prepare for general curricula, after which it was expected that they would be transferred to general schools.{mospagebreak}
By the mid-1990s, GoI initiated the District Primary Education Programme (DPEP) and its subcomponent known as the Integrated Education of the Disabled (IED). The main aim of DPEP has been to universalize primary education, including ensuring that CSN do not get sidelined in the process of expansion. Given that micro-planning has been a key element of DPEP, the Center offered states assistance to help plan execution of the IED. At present, DPEP is implemented in 23 districts of 3 states (Rajasthan, Orissa and West Bengal). Over 600,000 children with special needs have been enrolled in regular schools under the program.
The PWD Act itself was an important intervening policy development in education. As discussed in Chapter 7, its position on a rights-based entitlement to basic education was clear, and consistent with India’s international commitments on education of CWD (see Box 4.1). At the same time, its guidance on modalities for ensuring realization of the right was less so, with all options for delivery of education for CWD allowed for and not as much specific guidance on which was the priority mode anticipated and in what circumstances other modes would be appropriate. Just as importantly, it gave no guidance on who should take the decisions on the most appropriate form of education delivery for a specific child with a disability: administrative channels, more locally representative bodies such as PRIs or VECs, parents of the CWD, or the role of the CWD themselves in taking such decisions.
SSA was launched in 2001, and it aims to provide eight years of uninterrupted, good quality education to children between the ages of 6-14 years, and to have all children in school, learning and completing primary and upper primary cycles by 2010. The framers of SSA came to an early realization that their objectives could only be met if the education of CSN was an important part of the program. The key provisions under the SSA for integrating and including children with special needs is through: (i) a cash grant of up to 1200 Rupees per CSN per year; (ii) district plans for CSN that will be formulated within the above prescribed norm and (iii) the involvement of key resource institutions to be encouraged.
A specific feature of SSA is a zero-rejection policy. This suggests that no child having special needs can be neglected, nor denied enrolment on the basis of such concerns. The PWD Act provides, however, a loophole in how this is defined in practical terms. It states that children will be educated in an “environment, which is best suited to his or her learning needs” and that it is possible that the special needs of a child compel him or her to be educated in special schools. Where possible, the decision on the appropriate form of education is taken jointly by resource teachers, parents, medical teams and regular teachers. SSA itself provides useful flexibility to the local levels in making this determination, with an emphasis on AIE/EGS schools and home-based support, all intended to bridge CSN into mainstream education. While SSA offers each district to plan for its own future and for that of its inhabitants, the centre is playing play a useful role in disseminating good practice to help districts make appropriate choices.
As in other areas of service delivery, many of the issues discussed in the chapter reflect broader challenges in an education system which is grappling with issues of quality and drop out for children without specific needs even at the primary level. Many of the issues discussed with respect to CWD are thus more acute manifestations of broader challenges. The chapter seeks to identify key constraints on improving participation and learning outcomes for CWD, but equally acknowledges that the agenda is a medium term – in some cases long term – one, which requires prioritization and sequencing in the face of limited institutional capacity, and often constrained resources. Equally, it raises difficult trade-offs for those responsible for allocation of public resources for education. While Indian law and policy are clear in the commitment to the right of all children to basic education, in practice difficult issues arise. For example, if a given fiscal allocation aims to maximize enrollment, minimize drop-out and improve quality of education for all children, there may be tough choices in cases where the resource requirements for CWD are higher than for other children and bringing CWD into the system implies that greater numbers of non-disabled children do not enroll or drop out as a result. This is an area where a rights-based approach and that of economists and utilitarians can conflict.
However, they need not. International evidence suggests that the educational outcomes of non-disabled students can also be improved by inclusion of CWD in integrated classes. While more evidence from developing countries is needed, evidence from Canada and the USA at both pre-school and basic education levels found improved outcomes for non-disabled students from integrated learning. 2 Studies in India on the issue are to date lacking, but evidence from a pre-school study in the slums of Mumbai found that a range of developmental indicators for non-disabled children also improved significantly following the inclusion of disabled children.
Indian and International Policy Developments on Education of CWD
The education of children with disabilities and special needs in India was initiated in the late 1800s, with the establishment of special schools for the Deaf in Bombay in 1883, and for the Blind in Amritsar in 1887. By 1900 numerous special schools for the visually and hearing impaired children were set up across the country. This initiated the tradition of special schools in the country and till the 1970s, this was the dominant mode of service delivery for children with special needs (CSN). 4 It was only in 1974 that the scheme on Integrated Education of Disabled Children (IEDC) broke new ground by stressing the need for educating children with mild to moderate disabilities in regular school settings. However, the tensions between the role of special and general schools for CSN continues today, even after the widespread recognition that inclusion is seen as a more effective educational and social strategy in most cases.
The National Policy on Education (1986) brought the fundamental issue of equality for CSN to the forefront. 5 It stated that the “objective should be to integrate physically and mentally disabled people with the general community as equal partners, to prepare them for normal growth and to enable them to face life with courage and confidence”. While the NPE helped set the stage for further integration and inclusion, only in 1990 did the government provide teeth to the policy through the adoption of the Plan of Action (POA). The POA ambitiously committed to universal enrolment by 2000 for both children with and without disabilities. It also strengthened the NPE by demanding that CSN be educated only in regularly schools and not in special schools as had been allowed earlier. The placement principle for CSN in effect relegated special schools to the status of bridge schools. Children in these schools were expected to obtain training in non-curriculum areas, to help them prepare for general curricula, after which it was expected that they would be transferred to general schools.{mospagebreak}
By the mid-1990s, GoI initiated the District Primary Education Programme (DPEP) and its subcomponent known as the Integrated Education of the Disabled (IED). The main aim of DPEP has been to universalize primary education, including ensuring that CSN do not get sidelined in the process of expansion. Given that micro-planning has been a key element of DPEP, the Center offered states assistance to help plan execution of the IED. At present, DPEP is implemented in 23 districts of 3 states (Rajasthan, Orissa and West Bengal). Over 600,000 children with special needs have been enrolled in regular schools under the program.
The PWD Act itself was an important intervening policy development in education. As discussed in Chapter 7, its position on a rights-based entitlement to basic education was clear, and consistent with India’s international commitments on education of CWD (see Box 4.1). At the same time, its guidance on modalities for ensuring realization of the right was less so, with all options for delivery of education for CWD allowed for and not as much specific guidance on which was the priority mode anticipated and in what circumstances other modes would be appropriate. Just as importantly, it gave no guidance on who should take the decisions on the most appropriate form of education delivery for a specific child with a disability: administrative channels, more locally representative bodies such as PRIs or VECs, parents of the CWD, or the role of the CWD themselves in taking such decisions.
|
International policy development on education of children with disabilities
There has been a gradual – though by no means linear – strengthening of international commitment to inclusive education of CWD over the past 2 decades. India has been an important participant in these developments, and its own policy development in large part tries to incorporate its international commitments into domestic policy on IE. Some of the major milestones have been: The 1989 Convention on Rights of the Child noted that “Parties shall respect and ensure the rights set forth in the present Convention to each child within their jurisdiction without discrimination of any kind, irrespective of the child’s or his or her parent’s or legal guardians’ race, color, sex, language, religion, political or other opinion, national, ethnic or social origin, property, disability, birth or other status.” While a general base, it was an important step in reaffirming the right to education of CWD. However, unfortunately, the EFA declaration in Jontien in 1990 failed to mention explicitly the right of CWD to education. The failure explicitly to mention CWD in Jontien led to the Salamanca Declaration of 1994, which had an exclusive focus on children with special needs in the context of EFA. The Salamanca Statement and Framework for Action has the most definitive statement on education of children with special needs. Ninety-two countries (including India) endorsed the Salamanca statement requiring that “ordinary schools should be equipped to accept all children, regardless of their physical, intellectual, emotional, social, linguistic or other conditions”. The declaration also states that “Educational policies at all levels,. . should stipulate that children with disabilities should attend their neighborhood school, that is, the school that would be attended if the child did not have the disability”. The Declaration also commits that children with disabilities and special needs must have access to regular schools which should accommodate them within a child-centered pedagogy capable of meeting these needs. Unfortunately, despite the Salamanca Declaration, the EFA declaration in Dakar in 2000 again failed to mention CWD. Girls, ethnic minorities, and the poor are explicitly mentioned in the Declaration, and there remains a commitment to education for all, but Dakar represents a missed opportunity on IE. Hopefully, such stop-start initiative on IE will end with the recently-approved UN Convention on the Rights of Persons with Disabilities. Article 24 of the Convention very clearly recognizes the rights of CWD to inclusive education. The key provisions are as follows: “States Parties shall ensure that:
|
SSA was launched in 2001, and it aims to provide eight years of uninterrupted, good quality education to children between the ages of 6-14 years, and to have all children in school, learning and completing primary and upper primary cycles by 2010. The framers of SSA came to an early realization that their objectives could only be met if the education of CSN was an important part of the program. The key provisions under the SSA for integrating and including children with special needs is through: (i) a cash grant of up to 1200 Rupees per CSN per year; (ii) district plans for CSN that will be formulated within the above prescribed norm and (iii) the involvement of key resource institutions to be encouraged.
A specific feature of SSA is a zero-rejection policy. This suggests that no child having special needs can be neglected, nor denied enrolment on the basis of such concerns. The PWD Act provides, however, a loophole in how this is defined in practical terms. It states that children will be educated in an “environment, which is best suited to his or her learning needs” and that it is possible that the special needs of a child compel him or her to be educated in special schools. Where possible, the decision on the appropriate form of education is taken jointly by resource teachers, parents, medical teams and regular teachers. SSA itself provides useful flexibility to the local levels in making this determination, with an emphasis on AIE/EGS schools and home-based support, all intended to bridge CSN into mainstream education. While SSA offers each district to plan for its own future and for that of its inhabitants, the centre is playing play a useful role in disseminating good practice to help districts make appropriate choices.
The year 2005 saw the most recent and comprehensive policy push from GoI on education of both children and adults with disabilities, in the form of the Minister of HRD’s Policy Statement in March 2005,7 followed by a year long development of a national Action Plan for Inclusion in Education of Children and Youth with Disabilities. 8 The main objectives of the Action Plan are set out in Box 4.2. The Plan should – if effectively implemented – provide major impetus to improving educational outcomes of CWD. At the same time, the draft Plan and consultations around it suggest that there will remain major challenges in promoting institutional coordination within and between levels of government and administration, and in developing genuine partnerships with NGOs and civil society. This is part due to an absence of a comprehensive diagnostic of existing initiatives during the Plan’s development.
|
National Action Plan for Inclusion in Education of Children and Youth with Disabilities
The main objectives of the Action Plan will be to:
|
It is clear that education policy in India has gradually increased the focus on children and adults with special needs, and that inclusive education in regular schools has become a primary policy objective. The following section examines the extent to which these policy commitments are being met in practice in the educational attendance and attainment of CSN.
Educational profile of PWD
While policies are important, it is educational outcomes that matter. This section describes current data on educational outcomes of CSN and PWD. Overview statistics on both the educational attainment of PWD and the current school attendance rates of CWD in basic education were presented in Chapter 1. It is very clear that both educational attainment of all PWD and current attendance of CWD are very poor and far below national averages. This section develops the picture from Chapter 1 with more detail on CWD educational performance, mainly relying on NSS sources. The focus is primarily on children in general education.
- Literacy rates of all PWD: Chapter 1 showed the high illiteracy rates of PWD across disability categories. It is also possible to analyze illiteracy rates of all PWD by the self-declared extent of their disability. This is presented in Figure 4.1 from NSS. The findings run in the expected direction. Almost three quarters of those with severe disabilities are illiterate, and even for those with mild disabilities, the illiteracy rate is around half. 10 For the severely disabled, just over 10 percent have achieved middle school or higher education, while even for moderately disabled people the share is only 20 percent. Table 4.1 examines the same data for children currently of school going age, and show that the situation has not improved at all for children in the current generation with severe disabilities.
Illiteracy rates are very high for all PWD, but extreme for those with severe disabilities
Figure 4.1: Illiteracy and primary attainment rates for all PWD, 2002
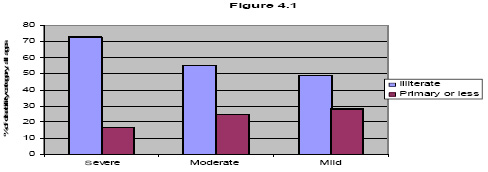
Source: NSS, 58th round. Bank staff estimates. - Literacy and attendance for children with disabilities: Figure 4.1 presents attainment data for the entire PWD population. For policy purposes, the more immediate focus has tended to be on current school age children and improving their educational attendance. Chapter 1 showed that around 38 percent of CWD aged 6-13 are out of school, with the rates much higher for certain disabilities. Figures 4.2 and 4.3 below track the school attendance of CWD between the ages of 5 and 18 by rural/urban and gender from 2002 NSS. Several points emerge:
- across all CWD, attendance at school never rises above 70 percent for boys and around two thirds for girls, confirming the SRI data on non-attendance from Chapter 1. These rates also compare very unfavourably with the age-specific rates for all children, which for boys peak at over 90 percent (at around the same age), and for girls at close to 90 percent.
- significant gender differentials among CWD do not emerge till around age 12. This shows a marked difference to the general school age population, for which boys’ attendance rates remain 8-10 percentage points higher than girls’ throughout the basic education cycle. 12 The conclusion would seem to be that the negative attendance impacts of disability are diluting the gender discrimination in basic education which one sees for non-disabled children.
School attendance of both boys and girls with disabilities is low, but gender differentials less than for non-disabled children
Figure 4.2: School attendance of PWDs, 5-20, by age and gender
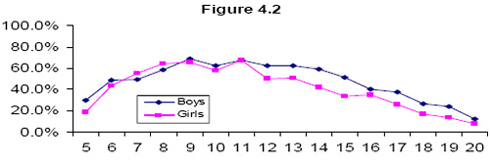
Source: NSS, 58th round. Bank staff estimates. - as expected, attendance rates in urban areas for CWD are higher than rural, but even at peak attendance never exceed 74 percent in urban and two thirds in rural areas. This can be compared to figures from the same NSS round for all children in Figure 4.4, which indicate much higher age specific enrollment rates for both rural (close to 90 percent) and urban (over 90 percent) children without disabilities.
School attendance for CWD in rural and urban areas is far lower than for other children throughout school age
Figure 4.3: School attendance for PWD, 5-20, by age and area
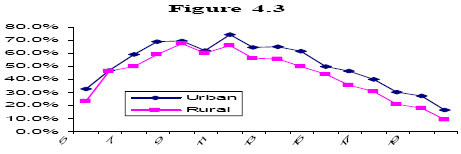
Source: NSS, 58th round.
Figure 4.4: School enrollment of all children by age and location, various years
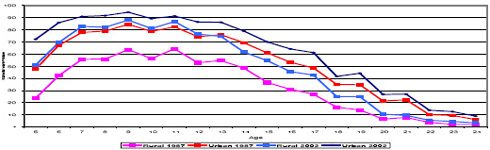
Source: World Bank (2006), based on NSS, 43rd, 50th, 55th and 58th rounds
As for the entire PWD population, it is also possible with NSS to look at both school attendance and current levels of educational attainment by severity of disability for those currently in school age. This is presented in Table 4.1 below for children 5-14 (the broad target age for basic education in India). Several points emerge:
- almost three quarters of children with severe disabilities are illiterate and the same share do not attend school.
- at the other end, close to one third of children with only mild disabilities are not in school. These are children who need no aids/appliances to participate, and should in principle not be significantly more difficult than other children to bring into the school system.
- across all levels of severity, CWD very rarely progress beyond primary school.
Table 4.1: CWD education attendance and attainment by severity, 2002
| Educational indicator | Severe PWD | Moderate PWD | Mild PWD |
| Goes to school | 25.7% | 56.3% | 67.9% |
| Illiterate | 72.2% | 42.6% | 34.9% |
| Primary or less | 26.4% | 52.0% | 58.2% |
| Middle | 1.5% | 5.3% | 6.8% |
| Secondary | 0.0% | 0.1% | 0.0% |
| Higher | 0.0% | 0.0% | 0.0% |
The above figures focus on national averages. Differences in CWD attendance can also be seen. This is shown in Figure 4.5 for CWD 6-13 years old. In even the best performing major state (Karnataka), almost a quarter of CWD are out of school, while more than half are out of school in states such as Madhya Pradesh and Assam. 14 There does not appear to be any correlation between the state-specific general out of school rate and that of children with disabilities, nor any clear pattern in CWD rates between state income levels and outcomes. Perhaps the most obvious point is that even states with excellent outcomes on their general child population such as Kerala and TN have stubbornly high out of school rates for CWD. Thus in Kerala, CWD account already for 27 percent of out of school children, and in TN for over 34 percent of all out of school children. This underlines the increasing importance of getting CWD into school if even well-performing Indian states are to achieve the education MDGs.
Out of school rates for CWD are high in all states and CWD account for a higher proportion of all out of school children as overall attendance rates increase
Figure 4.5: Share of 6-13 year old CWD and all children out of school, 2005
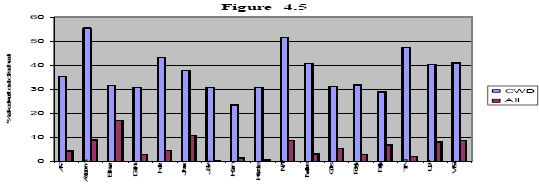
Source: SRI survey, 2005.
The other obvious aspect of educational attainment is to look at specific categories of CWD. This is shown in Figure 4.6. It is clear that illiteracy is high among all categories of disability, and extremely so for children with visual, multiple and mental disabilities. The numbers also rebut a common assumption that poor educational outcomes of CWD are a function of low intellectual capacities among children with mental impairments. At the same time, locomotor disabled children stand out as having substantially lower illiteracy rates than other CWD. This is explainable in part by the fact that less curricular or learning material adaptations are needed to promote inclusive education for locomotor disabled compared other categories of disabled children are required, but are also driven by family and community attitudes.
Illiteracy rates are very high among all CSN, though lower for children with locomotor disabilities
Figure 4.6: Share of Illiterate of 6-13 year old CWD by disability category, 2002
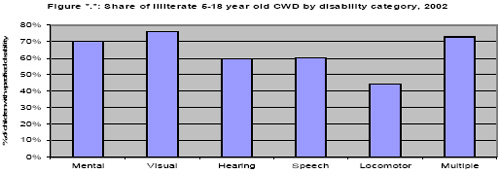
Source: NSS, 58th round. Bank staff estimates.
(iii) Where are CWD going to school ? This has several elements – whether CWD are attending regular or special schools, whether they are attending public or non-government schools, and for those in the government system what proportion of CWD are receiving alternative forms of education. This can be pieced together from several sources. On the issue of regular or special school, the NSS indicates that the overwhelming majority of CWD attend regular rather than special schools. Around 70 percent of disabled children and young adults aged 5-20 have ever attended school in their lives. Of these, fully 90 percent have attended a regular school. The figures for those currently attending school are very similar and are shown in Table 4.2, with nearly all 5-18 year old CWD who are in school attending regular schools. This brings home clearly that the choice facing most CWD is whether they are out of school or in regular school, and hence the necessity of promoting inclusive regular schools. The NSS also provides insight into why CWD are not enrolling in special schools. The picture is somewhat ambiguous, with a fairly even split between clear supply side factors such as lack of any or accessible special schools, clear demand side factors such as lack of parental interest and economic reasons, and factors related to the child’s disability which are hard to interpret.{mospagebreak}
Table 4.2: Share of CWD attending regular and special schools, 2002
| Currently attending regular school | Currently attending special school | |
| 5-14 years | 94.3% | 5.7% |
| 5-18 years | 94.8% | 5.2% |
Source: NSS, 58th round. Bank staff estimates.
A second important element of the educational attendance of CWD is whether they are in private or public schools and how that compares to children without disabilities. This is not available in NSS unfortunately. 16 One source is the UP and TN village survey and results from this are presented in Figure 4.7 below. The important feature in the results is not so much the absolute levels of public and private enrollment in the two states (which reflect quite localized supply and demand factors), but the relative rates of public and private enrollment among CWD and non-CWD. The share of CWD in private schools in rural UP and TN is only slightly less than for children without disabilities. Given the very low rates of special school attendance, this can be assumed not to be a special school effect only. The result is interesting in that parents of CWD who are in school seem equally willing to make the investment in private education despite the fact that labor market outcomes of PWD are so obviously worse.
Share of CWD and non-CWD in public and private schools among those attending, UP and TN, 2005
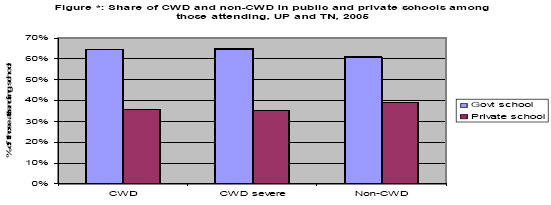
Source: UP and TN village survey, 2005.
A final element on CWD attendance is what proportion of those in the government education system are attending alternative schools. SSA data for 2006 indicate that around 3.0 percent of identified PWD are in EGS/AIE schools, and a further 2.4 percent in home-based education settings, the latter in particular a notable improvement from 2004/05. 17 In both cases, there is a strong statewise concentration, with many states reporting no CWD in either form of education.
(iv) Impacts on schooling of a disabled family member: The above discussion focuses on children with disabilities themselves. A further important issue is the extent to which having a child with a disability in the household may impact the educational attendance of other children in the household. In principle, this could be estimated from the NSS, though such analysis has not yet been undertaken. Pending that, the UP and TN survey asked directly about the role of siblings in caring for family members with disabilities and its impact on school attendance. The results are reported in Table 4.3. Encouragingly, they are not dramatic (though see the employment chapter for results on caring time of adults, which are more significant). Only around 5 percent of children with disabled members sometimes stay home to assist them, and of those only around 7 percent do so every day. Nonetheless, the impacts in the relatively small share of households affected should not be dismissed: half of households where a child does miss school require one or more days a week of school missed to assist disabled family members in the home.
Table 4.3: Children missing school to care for disabled family members, UP and TN, 2005
| Proportion of PWD households | |
| Share of HH where child sometimes misses school to assist disabled family member | 5.2% |
| Of which: | |
| Every day | 7.1% |
| More than one day a week | 21.4% |
| About one day a week | 21.4% |
| At least one day a month | 32.1% |
| Other | 17.9% |
Source: UP and TN village survey, 2005. Bank staff estimates.
Despite the move to more inclusive educational policies, clearly the educational outcomes of children with disabilities are substantially lagging those of the general population. This suggests that education of CWD is experiencing implementation problems which are characteristic of many areas of public policy in India. The following section explores the performance of key programs to explore the factors driving these outcomes.
Public Interventions to Promote Education of Children with Special Needs
Given the poor educational outcomes of CWD, this section explores several aspects of implementation of public programs to support inclusion of CWD, and of the general government school system which are relevant to educational outcomes of CWD. There are a range of institutional, fiscal/financial, and learning-related factors where there appears significant scope for improving the ways in which the education system promotes educational outcomes of CWD. Some of them are common to all children, but others are specific to CWD.{mospagebreak}
- Institutional Issues in Special Needs Education: Before performance in key programs for CWD, it is useful first to review the institutional arrangements with respect to education of CSN. This is an area that remains problematic in India. There are several institutional divisions of labor in the education of CSN which contribute to a lack of coherence in delivery systems.
The first split in the delivery system for special needs education is between the MHRD - which is responsible for the general education system - and the Ministry of Social Justice and Empowerment, which remains institutionally responsible for special schools. This division of labor seems philosophically a remnant of the earlier approaches where CWD were viewed as welfare cases and not like other children. It would also appear to act as an institutional brake on fuller interaction between special schools and the regular schooling system, so that the resource school model for special schools is more difficult to promote. Finally, such a division is increasingly out of step with good international practice in education of CWD.18 A UN survey of member states in the 1990s found that 96 percent of countries placed education of CWD under their education ministries, though in 58 percent of cases it was a shared responsibility.
A second split relates to teacher training, with the Rehabilitation Council of India responsible for special needs teacher training and MHRD which is responsible for general teacher training. Following the RCI Act in 1992 and amendment in 2000, the RCI now has wide-ranging set of objectives. These include regulating, training policies and programs, standardization of training courses for professionals and prescribing minimum standards, providing institutional recognition and conferring the rights to award degrees, diplomas and certificate courses for professionals in the country (and extending reciprocal rights to institutions outside of India), and in maintaining a Central Rehabilitation Register for professionals. There remains a basic split between the roles of MHRD and RCI in pre- and in-service training for both regular and special needs teachers which contributes to a lack of coherence in the teacher training regime for inclusive education.
A third split relates to lack of coordination and duplication of efforts in early identification of children with special needs. Most states use teachers and anganwadis for early identification. Information on the number of children is captured through what is referred to as household survey. 19 Before the survey is conducted, the anganwadis are oriented on specific formats that are to be used for the survey and have been developed independently by both DWCD and Elementary Education departments. The DWCD format is more comprehensive as it covers all persons with disabilities (PWD), and not just children from 5-13 years of age. The input- driven planning process adopted for SSA records the total number of children identified as being disabled, the number assessed, and the number enrolled in regular schools. Almost no other information is provided on early identification, assessment or enrollment, though MHRED notes this as a strategic choice so as not to overburden teachers. The end result is both an overload of the workers carrying out CSN identification and a database in the education system which can not be considered reliable. As a result, states are involving NGOs more in identification, with 10 SSA states using them in this role as well as their other functions.
A fourth institutional challenge has been to promote convergence between government and NGO/community roles in education of CWD. All the programmes under the Department of School and Mass Education have involved NGOs in the implementation of inclusive education programme. Currently, more than 530 NGOs are involved in some capacity in SSA in 26 states. However, the ongoing challenge is to give NGOs a broader role in promoting inclusive education in partnership with the state. NGOs are now involved in assessment camps and training of teachers, as well as a range of other functions, including bridge course, provision of home-based education, providing resource support, development of TLM and other activities.20 Deepening their role in every aspect of inclusion at each level (state, district, block, cluster, village and school) is an ongoing effort on the part of the Departments of School and Mass Education. In addition, there remains a largely undefined roles for grassroots institutions which could play an important role in promoting inclusion of CWD, including SHGs, Village Education Committees (VEC), Parent Teacher Association (PTA), Mother Teacher Association (MTA), anganwadi workers, Mahila Swasthya Sanghas (MSS), members of cooperative societies, and community based Local Bodies.
The above institutional issues in delivery of different aspects of education for PWD are by no means exhaustive. Similar divisions can be seen at higher levels in the division between vocational and higher education. However, even at the basic education level, such institutional lack of convergence remains a hindrance to promoting education of CWD. - Financial performance of public interventions for education of CWD: As noted in the policy section, the IED – now within SSA primarily – is the central public intervention to support education of CWD. This section reviews the evidence on its financial performance. Currently, under SSA the allocation per CWD is Rs.1200 per annum. While the norm is child-based, financial allocations are aggregated at district level. Currently – despite the clear policy commitment under SSA - there is no way of guaranteeing that a child with a disability, who attends school in a particular district, and is eligible for an assistive technology device, will actually receive this. This is because the funding is district or at best school based. The funding follows the location and not the child, thus there is no scope for school choice among children with special needs. Survey-based evidence on the coverage of assistive devices (see health chapter) clearly indicates a significant remaining agenda in this area. Box 4.3 compares the three main models of funding education of CWD internationally and their relative merits.
Box 4.3: Main models of public educational financing, with different impacts on CWD and IE:
Internationally, there are three main models for financing education of CWD, each of which has different incentive structures and impacts on both inclusion and educational outcomes. The models and their main features and pros/cons are:- Child-based funding – based on headcounts of CWD, as outright grant to regions, pupil-weighted schemes, or census funding based on total students and assumed share of CWD. This is the most frequently used model internationally and the one followed under SSA. However, there are issues with the model including: (i) concerns on the focus on the disability category of the child vs. actual learning needs and costs. Thus the system is necessarily mechanical rather than needs-based; (ii) the model can be costly where individual diagnosis is required; and (ii) evidence from the EU suggests integration outcomes for CWD are worse that other approaches.
- Resource-based models (aka “through-put” models), where funding is based on services provided rather than CWD/student numbers. Typically, this model also mandates units of instruction/programs. Overall, there is evidence of an OECD trend towards these models, which are found to encourage local initiatives to develop programs for CWD. There are, however, concerns on disincentives for schools when CWD progress and funding is reduced. To work well, this approach should be accompanied by some link to outcomes.
- Output-based models: These are based on student learning outcomes or some other output. While desirable in principle, there has to date been very limited experience with this approach, (e.g. US No Child Left Behind Act, with financial and accreditation sanctions for failure to meet student achievement standards; UK “league tables”). There are concerns of a natural bias against inclusive education, due to concerns re CWD behind grade level dragging down school average scores. Equally, the circumstances for “failure” are often beyond the school’s control (e.g. student absenteeism; unadapted curriculum).
Figure 4.8 presents the share of total expenditure by major states on inclusive education in 2004-05 from SSA. Overall, the spending share on inclusive education in SSA is low, at only 1 percent nationally. However, there is major variation in IE spending share between states, ranging from over 5 percent in Kerala to well below half a percent of SSA spending in MP, Jharkhand, West Bengal and Rajasthan. Equally, expenditure execution on IED was until very recently low (under 40 percent in 2004/05) and also exhibits huge variation across states, with states such as TN, Karnataka and Assam at very high execution rates, while others perform very poorly (in West Bengal, under 10 percent execution – Figure 4.9) One positive element of the picture is that SSA IE expenditure execution nationally increased from only 26 percent in 2003/04 to around 65 percent in 2005/06, and that states such as Assam and MP showed dramatic improvements in execution over the two years.
Inclusive education spending is a low share of SSA, but some states perform much better than others in terms of expenditure execution
Figure 4.8: Spending on IED as share of total SSA, major states, 2004-05
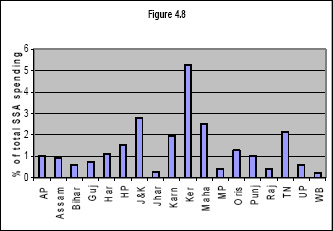
Figure 4.9: IED spending execution as share of allocation, 2004-05
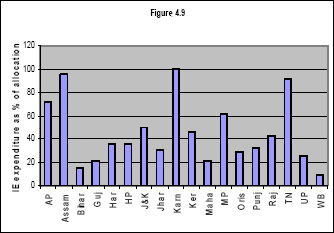
Source: SSA.
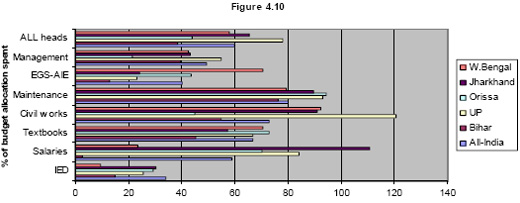
A second aspect is expenditure execution on IED relative to other heads of SSA spending. Figure 4.10 provides insights on the expenditure performance on IED within SSA for all-India and for five of the poorest states (Bihar, Jharkhand, UP, Orissa and West Bengal). It is clear that the relative expenditure performance on inclusive education was initially very poor (not much over half the average execution rate across all SSA spending), and consistently so across states. This is in contrast to most other heads which are either consistently well executed (e.g. civil works and maintenance) or exhibit strong variations across the states (e.g. salaries). At the same time, recent performance shows marked improvement, with sharp improvement in execution even in poor states. For example, in 2005/06, Orissa nearly doubled execution to 54 percent, UP leapt from 25 to 86 percent execution, and West Bengal went from under 20 to 49 percent.
SSA expenditure execution on inclusive education is poor, nationally and in the poorest states
Figure 4.10: IED expenditure execution as share of allocation for SSA, 2004-05
Overall therefore, it appears in many states that failure to execute spending for IE is one factor in driving the poor attendance of CWD. However, poor resourcing is not by any means the only factor contributing to both poor attendance of CWD and poor educational outcomes. The following sections review a number of other factors which are important. - Making schools inclusive for CWD: A number of factors driving poor educational outcomes of CWD can be grouped under the heading of accessibility and inclusion. There are several elements of making schools and learning accessible for CWD. They include:
- an effective system for early identification of children with special needs, both in terms of medical assessment and in terms of identifying their special learning needs and potential
- attitudes of parents, communities and education service providers and administrators which promote inclusion of CWD and promote them realizing their potential
- physical accessibility of schools, not only the school premises and facilities but also accessibility from the child’s home, which brings in issues like transport systems and roads.
- access to appropriate curriculum and learning materials which are adapted to their learning needs of CWD, both in content and format
- provision of financial incentives and aid/appliance support for CWD to facilitate their participation in regular schooling
- presence of teachers and education administrators who are sensitized to the rights and needs of CWD in education, and are equipped with basic skills and access to resource personnel and materials who can supplement the skills of general teachers
- encouraging a special education system which facilitates inclusive education through greater reliance on the community (e.g. through CBR), rather than inhibiting it through over-professionalization.22
- development of coherent government strategies for promoting inclusive education, which in particular take greater account of the important roles of NGO and community organizations.
- an effective system for monitoring and evaluating the educational attendance and attainment of CWD, preferably integrated with the general education M and E system.
This section deals with the above elements of accessible and inclusive education for CWD. Many of the principles necessary to promote inclusion are reflected in recent policy documents of GoI, including the draft Action Plan. However, implementation has typically fallen short of policy commitments, in many cases far short. Implementing coherent strategies for inclusive education is one of the greatest challenges facing education systems in both developed and developing countries. Capacity, resource, and attitudinal constraints make the challenge even greater in India. Making progress on the above agenda will take considerable time. Nonetheless, there are many effective and promising experiences in India which suggest that significant improvements in inclusive education are possible in ways that are consistent with the constraints that India faces. It is also important that the system succeed on the basics first - primarily identification of CWD and getting them into some form of education from the earliest possible point.
- Identification of CWD: The bottom-up approach to planning adopted under SSA is expected to provide a clear picture on how many children will need special assistance to participate in the schooling system. Since district-level funding is tied to the identification of children with special needs, the designers of SSA have attempted to define how the process of identification should be done. GoI has developed a simple set of definitions and a disability-specific checklist to help determine children with mild to moderate disabilities.
Once children have been identified as disabled, an assessment is undertaken to determine the nature, type and extent of disability. This is done by a team comprising of doctors, eye and ENT specialists, and general and resource teachers. The child is then placed in a particular school-type. While the guidelines calls for all children with disabilities to be placed in regular school settings, they also permit the placement of children in special schools, AIE/EGS centers, distance learning centers and home-based education if it is decided that the child is not in a position to participate in regular school, and the interventions they require will be beyond those that can be offered in a regular school even with a trained and qualified teacher. This reflects the broader transition from a special education to inclusive education model.
There are three key issues with early detection and identification of CWD for education policies:- technical and logistical difficulties in early identification. As noted earlier, some of the issues relate to institutional lack of coordination and duplication. A second aspect of this is the functioning of disability identification camps, which achieved at best partial coverage of CWD.23 A further concern with testing of younger children is that they need specific preparation for testing, and that the instruments and personnel needed for these may not be readily available in many parts of India.
- there are large discrepancies in the number of CWD identified between census data, school-based records through DISE, and PAB survey aggregates used for the preparation of SSA annual prospective plans. For example, PAB data find only 1.54 percent of children identified as having special needs nationally, though this is a significant improvement from only 0.35 percent in 2002/03. Even more significantly, there are unreasonably low shares of children identified as having special needs in specific states. For example, data for 2005-06 suggest that only 0.31 percent of children in Rajasthan had special needs and 0.7 percent in UP. In contrast, states such as Maharashtra had 2.45 percent and HP around 2.3 percent of children identified with special needs. In contrast, census data on 5-14 year old children with disabilities nationally suggests that 2.2 percent of children have disabilities. On a statewise basis, the differentials are even more dramatic in several cases, e.g. the number of children identified by PAB in Rajasthan as disabled for 2005-06 was less than 15 percent of the number of 6-14 year old disabled children identified in the 2001 census. For UP, the PAB share was under 30 percent of the census figure. In contrast, states such as Maharashtra and Kerala have SSA CWD numbers well above the census estimates. The discrepancies between SSA and census sources suggest major challenges for government in identifying children with special needs. Figure 4.11 provides comparative figures for several states on the share of children identified as disabled through SSA and the estimate of all CWD in the 6-14 age cohort as per the census.
The numbers of CWD identified by SSA relative to census numbers is below half nationally and far less in some states
Figure 4.11: CWD identified by SSA in 2005 as share of 6-14 year old CWD in census by state
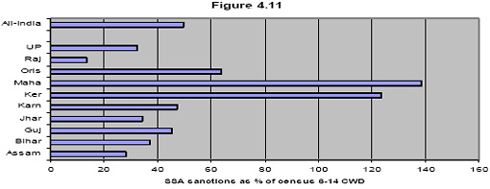
Source: SSA and 2001 census (Bank staff estimates based on Rajan). - there have been concerns expressed from educators that identification of CWD is viewed more from a medical perspective and does not focus sufficiently on the learning needs of children with special needs. For example, although medical camps were initially envisaged to be used for certification and identification, increasingly in states like Andhra Pradesh, they are being used to identify children suitable for corrective surgery (e.g. children with cleft palettes, etc.). In principle, such camps do address a broader range of needs, but in practice have supply side and other limitations.
- Attitudes to CWD: Even very poorly resourced systems can be inclusive if the attitudes of parents, communities and teachers are sufficiently supportive. Chapter 2 demonstrated that positive attitudes to CWD being included in regular schools were rare in rural UP and TN, and that there was virtually universal rejection of children with mental disabilities attending regular schools, even among both PWD and parents of children with disabilities. However, qualitative work found generally a more open attitude to inclusion among teachers.
There has been relatively little research on the attitudes of teachers towards the education of CWD in India. The existing research on teacher attitudes reveals mixed results. An initial study in the 1990s on the attitudes of administrators, special education teachers and general education teachers towards CWD found that over 50 percent of administrators had misgivings about their education in regular schools.25 Special and regular school teachers had more positive attitudes regarding integration of CWD in regular classrooms. Administrators however did agree that integration would benefit both children with and without disabilities. A later study on attitudes towards inclusion in Delhi found that almost four-fifths of teachers interviewed had an open approach to inclusion, although three-fifths felt that special schools would be better for CWD. The most recent study looked at the attitudes of general education teachers towards CWD and inclusion in Mumbai. The results are summarized.
Teacher attitudes to inclusive education in Mumbai
Parasuraman (2002) studied the attitudes of general education teachers towards CWD and inclusion in Mumbai. She specifically explored several demographic variables of teachers, such as, gender, age, income levels, experience, educational attainment, whether the person had a friend or a relative with disabilities, and the frequency and proximity of contact with this disabled person. She found that:- younger teachers (20-30 years old) and the most senior (50-60 years old) demonstrated more positive attitudes towards CWD, compared with the teachers in the 40-50 age group.
- there were no differential effects due to gender (although other studies have shown this)
- higher income groups have more positive attitudes than lower income groups (less than Rs.10,000).
- experience as a teacher demonstrates a pattern that is similar to age in that the youngest teachers (with less than 5 years of experience) and the oldest teachers (with more than 25 years of experience) demonstrate the most positive attitude towards CWD
- the more educated a person, the more positive their attitude is towards inclusion, thus, teachers with a master’s degree are more open to inclusion than are teachers with a bachelor’s degree or a high school certificate
- knowing someone with a disability was likely to influence thinking on inclusion positively
- however, knowing someone with a disability who was related to you did not have more of an impact than merely knowing someone with a disability, i.e., kinship did not result in more positive attitudes
- both the frequency of contact and the closeness of the relationship did not have any significant effects on positive attitudes towards inclusion of children with disabilities.
The UP and TN study asked CWD directly about their perceptions of attitudes of teachers and classmates towards them. The results were encouraging, with the bulk of CWD reporting some degree of support towards them in their schools, and only a small number reporting discriminatory attitudes. The results are presented in Table 4.4, with around 85 percent of classmates and almost 80 percent of teachers reported as being very or somewhat supportive.
Table 4.4: Attitudes of teachers and classmates of CWD in UP and TN were positive
Source: UP and TN village survey, 2005Share of CWD reporting teacher’s attitude as… Share of CWD reporting classmate’s attitude as… Very supportive 35.5% 50.4% Somewhat supportive 43.7% 34.5% Indifferent 6.7% 5.9% Somewhat uncaring 4.2% 5.9% Discriminatory 0.8% 0.8% Don’t know/can’t say 9.2% 2.5%
The limited empirical evidence thus supports the proposition that attitudes of educators towards inclusion of CWD are gradually improving. However, evidence from several states indicates less movement with respect to both general community attitudes and those of parents of CWD. GoI, in cooperation with the State governments, NGOs and other stakeholders have recognized the importance of this change in attitudes and have organized numerous maa-beti samelans, bal samelans, and other forms of interventions to help change attitudes. However, a more comprehensive approach is clearly needed. This is an area where Community-Based Rehabilitation (CBR) can play a potentially important role in mobilizing attitudinal change. - Teacher Training and Methods: As well as positive attitudes to inclusion, training of teachers in the principles and practices of inclusive education is an important element of making the school experience of CWD worthwhile. This covers both pre- and in-service training, for both regular and special educators. Box 4.5 outlines the broad contents of different IE training options. The impacts of such training are typically improved when educational administrators are also trained.
Given the overwhelming proportion of CWD in regular schools, the importance of training on special needs education for regular teachers can not be under-estimated. However, to date pre-service training of regular teachers includes no familiarization with education of special needs children. As a result, the effectiveness of in-service training is even more vital. As of 2004/05, the bulk of in-service training for regular teachers in SSA schools has been the orientation on IE as part of their mandatory 20 days in-service training per year, with around 40 percent of teachers having participated. The share of teachers who had undertaken the 3-5 day exclusive IE course increased also, from only around 12 percent of all teachers in 2004/05 to almost 30 percent by 2005/06. There is as usual large inter-state variation, with states such as Karnataka and Maharashtra having only 10-12 percent of teachers having had either form of IE training, while others such as Kerala, UP and Haryana had achieved very high coverage of teachers (e.g. in UP, more than half of teachers had had the 3-5 day course in 2004/05). However, the number of teachers undertaking the 45-90 day foundation course remained very low as of 2005, at less than 0.2 percent of all SSA teachers. 27 While the coverage of basic sensitization courses under SSA is growing, the penetration of RCI training has been negligible. As of 2006, RCI had trained a total of 27,252 personnel and professionals, or around 0.6 percent of total SSA teaching cohort.
In the area of teacher training, a key issue of debate is the role of RCI and its certification of training programs and trainers. There have been a range of criticisms of the RCI with respect to teacher training. The first is that its genesis and skills base tend more towards a medical mode of disability and that it is thus not well equipped to develop and certify training materials. Additional criticisms include: (i) the development of RCI rules and regulations have generally been done without any consultative process; (ii) punitive actions for failure to comply with articles within the Act; (iii) failure to draw a pragmatic line between the need for standardization in training and the need to promote wide coverage of service delivery and (iv) the need for a meaningful definition of a rehabilitation professional; and (iv) the inability for capacity reasons of RCI to monitor compliance.
While the legitimacy of RCI as the sole statutory body with authority to recognize training programs and confer degrees to persons specializing in special education is not questioned, an increasing number of trainers, care-givers and experts are questioning the need for a sole agency to be given such a large mandate, and whether the mandate should be shared by specialized agencies that exist across the country. The number of special teachers in the country is extremely small compared to the total number of regular school teachers. DIETS, SCERTS, other public and private teacher training colleges that offer courses on special education are all required to be certified by RCI. Given the tremendous imbalance in terms of the need for special education teachers and IE skills among regular teachers, the concerns of the profession seem worthy of closer consideration.
Training on IE for regular and special educators
In-service 1 day orientation on IE for regular teachers:- Concept of inclusive education
- Identification of CWD
- Classroom management of CWD
- Difference between integrated and inclusive education
- Types of special Educational Needs (visual impairment, hearing impairment, locomotor impairment, mental retardation and learning disabilities)
- Causes of disability
- Identification of CWD using a simple checklist
- Role of teachers in dealing with CWD
- Use and maintenance of assistive devices
- Rehabilitation in disability
Contents of Teacher Training of Special Schools- History of Special Education
- Anatomy and Physiology of eye/ear/brain
- Causes and prevention of disability
- Multi-Category teaching
- Plus Curriculum
- Guidance and Counselling
- Prevention
- Use of aids and appliances
- Preparation of teaching-learning material
- Educational implications of different kinds of disabilities
- Practice teaching
The modes of educational delivery anticipated under IED are diverse and on paper they are impressive. Box 4.6 outlines the main intervention menu that is anticipated under IED and from which states are supposed to develop state-specific strategies for the getting CWD into school and improving their educational outcomes. However, cases where the menu comes together in a coherent and well-executed strategy for IE are much more limited. - Incentives for CWD to go to school: National and state governments have a range of incentives for CWD to attend school, the most important being stipends. These were introduced only in 2002-03, i.e. seven years after the PWD Act, despite provisions in the Act for stipends. According to GoI, there are 32 states/UTs that provide some sort of scholarships/stipends to students with disabilities, typically up to primary or middle school (and in very few cases beyond secondary level). For primary education stipend varies from Rs. 5/- per month in Pondicherry to Rs. 200/- per month in Punjab. The CAG report notes that by mid-2003, the MoSJE acknowledged that it had not taken steps for dissemination of information on the stipend program.30 Consistent with this, anecdotal evidence suggests both a low level of awareness among CWD and their families of stipend possibilities and inadequate efforts on the part of the authorities to increase stipend coverage. There are no consolidated data on stipends available, so that it is difficult to examine the scale and impact of stipends.
Although a key feature of SSA, the provision of aids and appliances is achieved through convergence with other existing programs such as ADIP31, a scheme aimed at helping disabled persons by providing suitable, durable, scientifically manufactured, modern, standard aids and appliances. While assistive technologies are a right under SSA, they are in practice rationed, making them instead a privilege. While SSA itself has no excluding procedures, there are specific eligibility criteria under programs such as ADIP with which SSA converges that need to be met before becoming entitled to an assistive technology. Under ADIP, the CWD needs to be certified by a registered medical practitioner that he is disabled and fit to use the prescribed aid or device, and that he or she is in a particular economic bracket, and has not benefited for the same purpose in the past 3 years (1 year for children below 12 years of age). In principle, if states do not provide aids and appliances under such programs, SSA can provide equipment. In practice, the NSS results indicate that such interaction is not seamless and coverage gaps remain.
Service delivery modes for CSN in IED
Service delivery in IED can happen through a variety of mechanisms. The main modes of delivering integrated education services through DPEP and more recently SSA are:- integrated schools: in that there is a clear and significant departure from Special Schools under DPEP and although there has been continued expansion of special schools, largely under the ambit of the Ministry of Social Welfare, there has been a increased focus on inclusion in general schools.
- resource room model. The resource room allows for children to be educated in an inclusive setting, but with the provision for specialized attention when needed. For example, a child who is unable to access the regular curriculum due to a disability, can be taught the same in the resource room
- traveling teacher model is a model adopted initially to address the concerns of migrant children and for children in rural areas where sparsely populated areas may have difficulty ensuring the presence of a school. However, the itinerant teacher’s function is to be able to cover several schools at the same time, unlike the resource teacher who can at the most cover 2 schools.
- dual teaching (for slow learners) where children are provided with extra tutorials and over an extended period of time to ensure learning by these individuals
- learning corners are used in classrooms to help organize class material and to support the development of curriculum. These provide children with special needs to pursue on their own, in a child centered manner, the exercises done in the classroom at an earlier point in time
- distance Learning is already being carried out through the National Open School and the new EduSat satellite based school TV channels
- home based education is an option for children with severe or multiple disabilities, who are unable to participate in regular school. In this case, the school actually goes to the house
- additional resource teachers and sensitization of regular teachers,
- NGO involvement is a key feature of DPEP’s and SSA’s IED scheme. Several states have entrusted responsibility for IED services to NGOs working closely with the governments in those states.
- development of a model kit works in complement to the Learning Corners and Itinerant teacher initiative as it allows for well-developed modules to be given easily across several locations
- training of trainers and master trainer method.
The results of the UP and TN survey support claims that both the stipend and aids/appliances schemes are not to date working well. For aids and appliances, the results are supported by NSS findings also (Table 4.5). Almost three quarters of households with PWD were unaware of schemes for free aids and appliances, and less than 2 percent had benefited from them. For stipdends, almost half the PWD households were not aware that education stipends were available and only 4 percent had received them. A major problem appears to be lack of awareness of the existence of CWD stipends and possibilities for receiving aids and appliances. Analysis of NSS data suggests that failure to access aids and appliances matters for school attendance, with multivariate analysis from the 58th round indicating that CWD who have accessed aids and appliances are 30 percent more likely to be attending school.
Table 4.5: There is low awareness of possibilities for aids, appliance and stipends and very low shares of beneficiaries in rural UP and TN
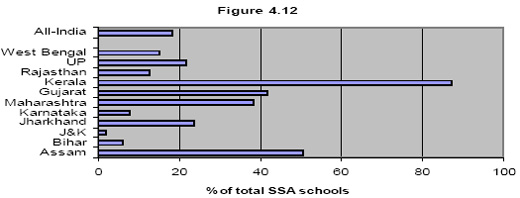
Source: UP and TN village survey, 2005Stipends to CWD for school Free aids, appliances and assistive devices Not aware 46.5% 72.3% Aware only 46.7% 24.1% Benefitted 4.4% 1.5% Denied 2.1% 1.8% - Physical accessibility of schools: Obviously a school has to be physically accessible to be inclusive. While typically this is thought of primarily in terms of ramps, other forms of increased accessibility for visually impaired and other CWD are equally important. Physical access includes not only the schools premises and classrooms, but core facilities such as toilets. Official statistics on “barrier free access” indicate that basic education in India is predominantly not physically accessible for many children with disabilities, though significant progress has been made in recent years. At the same time, the data also indicate that broadening the coverage of schools which are classified as barrier free is achievable, as the performance of states such as Kerala, Assam and Gujarat indicate. Figure 4.12 below reports the share of primary schools which are officially rated as barrier free in selected states in 2005. Only 18 percent of SSA schools nationally were considered accessible in 2005, and the share is as low as 2 and 6 percent in Jammu and Kashmir and Bihar respectively. Nor does the accessible share follow predictable patterns, with generally good performers like Karnataka and well-off states like Punjab with less than 8 percent of schools accessible. At the same time, progress is being made, with the figure for 2006 rising to around 35 percent.
The bulk of SSA schools are not accessible for CWD – nearly all in some states
Figure 4.12: Share of accessible SSA schools, 2005
Above and beyond schools themselves, there may be issues with CWD getting from home to school. This is an area where very little research exists, and one that is an issue that goes well beyond the needs of CWD alone. Nonetheless, difficulties with access to transport and/or simply difficult personal access may be much more pronounced for certain CWD. The UP and TN survey asked about access to public transport, and over 60 percent of PWD respondents reported difficult or no access to public transport due to their disability. - Accessible curriculum: To date there remains major differences in curriculum between special and regular schools. The current mode of delivery of such services in India is categorized into two sets. The first is the skills relating to what is called “Plus Curriculum” in special needs education curriculum. It is called Plus Curriculum as it is a specific curriculum for CWD intended to increase their access to the learning environment (for example, Braille, orientation and mobility for children with blindness, use of low vision aids and reading large print by children with low vision sight, speech, language and communication skills by deaf children, communication skills by children with cerebral palsy). They have to learn additional skills for fully participating in classroom learning activities and require additional time.
The other set of questions deal with adjustment of general curriculum to diverse educational needs arising out of disability, and use of additional learning resources and classroom management to improve access of all children in learning activities. The curriculum options for CWD in general curriculum/school settings are several:- follow the same curriculum as others, in principle maintaining equity in curriculum access. While in principle this is straightforward, this option still requires development of accessible formats of the general curriculum for children with specific disabilities (e.g. Braille books; visual learning materials for hearing impaired and autistic children). For the most part, such format adjustments have not been made on any large scale in the public system. 34
- adjustment or/and modification to special needs in areas which cannot be accessed despite assistive aids and additional learning material and aids
- substitution of curriculum content area by alternative content area
- deletion of specific curricular content area since it is not possible provide learning to a child with a particular disability.
An important point with respect to curriculum adaptation for CWD is that international evidence suggests that such adaptations can also have positive effects on the learning outcomes of non-disabled students also. While evidence from developing countries is lacking, an eight country OECD study found that adapted curriculum and pedagogy motivated by inclusion objectives resulted in improved educational outcomes for non-disabled students also. A simple example is greater reliance on visual teaching materials, which may be both necessary for hearing impaired students and beneficial for the learning of all students. Further analysis on this issue in India would be highly desirable.
All states have special provisions for CWD taking examinations. Writers are provided to blind students and other students who cannot write. The writer is to be a student from a class below the examinee, thus ensuring fairness in the process. While fairness is important, lower classmen and women may be more limited in their own understanding of subject matter and thereby be a poor substitute for a student of the same grade. Field work for this report revealed that the arrangement was characterized by mistrust between the examinees and the examining board. The earlier practice of allowing blind students writing in brail was replaced due to non availability of examiners knowing brail and time consuming and costly translation. The issue needs to be reviewed and alternative ways need to be found. For example, some subjects can be examined through audio mode and the use of computers and ICTs is also be considered.
Students are often allowed to take extra time to write their examinations, e.g. an extra half an hour is allowed to blind students with writers in Gujarat; AP provides CWD an extra hour to write exams. At present the decision is ad hoc. The Board also allows practical examination in peer pairs (a blind with a sighted) or the practical examiners individually attending and asking question with each step. While the rules are clear on allowing extra time for exams, the UP and TN study revealed that the rules may not always be implemented in practice, with three quarters of CWD reporting that they were not always given extra time to finish exams. - Strategies to implement IE obligations: Apart from the specific elements of IE promotion noted above, there is a need for overarching state (and lower level) strategies for implementing their obligations to provide education of CWD. However, most states to date do not have a strategy for resource support in the form of resource teachers or any other specialized support service required by CWD. While this is slowly improving in some states, it clear from the data that there remains a basic lack of IE delivery strategy in much of the country. The framework for SSA requires the appointment of a state coordinator for inclusive education, and all states/UT now have such a person in position. As a result, there are many initiatives and a growing number of resource teachers (around 4,693 in 17 states as of 2006), but such initiatives are not always guided by a longer-term strategy.
However, the experience of states like TN offer cause for hope. Tamil Nadu has rapidly raised IE expenditure execution from less than 10 percent in 2002/03 to 55 percent the following year and over 90 percent in 2004/05, largely due to a change in policies on how to handle the IE component of SSA. The state recognized the strong capacity and commitment among the NGO community to undertake this task, and the Department of School Education of GoTN tasked credible NGOs to undertake identification and intervention activities. As a result, it has been able to channel resources to these NGOs rather quickly. Not all states will have the existing disability and general NGO base of TN, but the capacity for major expansion in public-private partnership in IE is clear. The TN case points, however, to the importance of better understanding of NGO initiatives in inclusive education. This is addressed in Section D below. - Monitoring and Evaluation: A key feature of SSA is its focus on monitoring and evaluation of inclusive education practices for children with special needs and their performance in the schooling system. This includes quarterly national IE workshops, use of NCERT monitoring tools on attendance and learning achievement of CSN, joint review missions under SSA, and regular visits by the SSA technical support staff. In addition, there are 39 monitoring institutes across the country that look at all SSA interventions, including IE. At the state level, a number of states (including all southern states and a number of lagging states such as Orissa and UP) also rely on their IE resource teachers for monitoring, and in states such as Assam, GP level volunteers are also involved in monitoring. Finally, an impact assessment study on IE under SSA has been commissioned and should be a valuable resource.
While the commitment is there and regular data is collected on a range of IE indicators, analysis suggests that there are challenges in implementing the system, not least identifying all CWD. Very few evaluations have been fielded till date on whether the legislative and design aspects are working. The DISE data system for capturing participation of children with special needs in the schooling system has been in effect for about three years, but significant inconsistencies between DISE, NSS and census data suggest that the M and E agenda on IE remains far from complete.
While the areas above are all elements of an inclusive and effective educational strategy for CWD, it is also important to be realistic on what is feasible in what time horizon given the overall context of the basic education sector. The IE challenges above need to be viewed in the context of a basic education sector where enrollments have increased substantially in recent years, but there remain many challenges, including significant drop-out rates, crowded class rooms, issues with teacher absenteeism (e.g. a major study found around 25 percent of teachers absent, with around one third of those not engaged in other activities), concerns with the quality of teaching and approaches in learning curriculum, major challenges in assessing learning outcomes etc. There is a risk in such an environment that including CWD into the educational system is put in the “too-hard basket”. In that context, an absolute minimum should be fulfilling the commitment to identify CWD and get them into some form of school.
{mospagebreak}Non-government roles in education for CWD
The preceding section focused primarily on SSA/IED as the major public education initiative for CWD. However, education of children with special needs has a long tradition also in the non-government sector, and much of the most innovative work in education for CWD continues to happen outside the public system (or through partnerships where the government finances non-governmental service delivery). This section reviews NGO roles in education of special needs children in India, and assesses the potential for an expanded role for partnerships between government and non-government providers.
As with the government sector, the tradition of NGO education for CWD was one of special schools until at least the mid-1950s. To some extent, this strong tradition continues, both on an independent basis and through the work of NGO special schools funded through the MoJSE NGO grants. In 2003/04, MoJSE provided grants-in-aid to 657 NGOs for a total of Rs. 71 crores and for the benefit of 2.17 lakh people (though this was reduced to Rs. 67 crore in 2004/05). The bulk of this assistance went for residential and non-residential special schools for different categories of CWD. As can be seen, given the numbers of PWD covered by all MoSJE grants, it is clear that the more significant NGO activities are likely to be those carried out independently or as partners/executing agencies within mainstream education initiatives.
Since DPEP and increasingly in SSA, there is a stronger public policy of linking NGO schools for CWD with the mainstream education system, either as direct service providers of different forms, or as resource centres for regular schools. The overall concept of support is to strengthen linkages between general and special educators and educational establishments. The main NGO initiatives which are supported through SSA focus on four main approaches:
It is clear that NGO/government partnerships hold great potential for expanding outreach to and inclusion of CWD in mainstream education. However, more assessment is needed of the extent to which the standardized per child allocations under SSA can accommodate different types of interventions. Even in successful states like TN, there are concerns among NGOs that effective publicly-financed support from NGOs to CWD is being sustained through implicit subsidization from the operations of NGOs themselves. Governments will need to do more work on evaluating the real costs of different modes of inclusive education, as a policy commitment to meeting the individual and special needs of CWD needs to be set against both finite resources and a system of education budgeting which often lacks flexibility.
Even with increased and effective NGO involvement, the primary responsibility for guaranteeing the rights of CWD remain with governments. Increasing the involvement of NGOs needs to avoid the pitfall of education of CWD becoming a “residual” sub-sector. Integrating management of CWD education under the MHRD may be one channel for ensuring that this does not happen. Using NGOs both as advocates and as a source of expertise fore increasing the capacity of mainstream public systems is another key element of such a strategy.
Conclusions and recommendations
More than most areas of policy with regard to people with disabilities, the education sector has been relatively progressive in policy terms. It has also in principle committed to a progressive menu of options for delivering education to children with special needs. However, it is clearly struggling to turn policy into effective practice for a variety of reasons. It seems that there is a major need to get the basics right: identify children with disabilities more effectively; make the content and format of what they learn relevant and accessible; have resources available with adequate outreach to teachers and children; and work through various channels to convince families and communities that educating children with disabilities is worthwhile. However, all this needs strategic direction on inclusive education at state and lower levels of the system which in most states still appears to be lacking to date, though examples such as Gujarat and TN provide guidance on how this can begin to happen. More specific directions include:
Improving identification of children with disabilities and promoting access to schools: This is the absolute priority in the first instance, as without identification and some form of access, any qualitative efforts to improve the inclusiveness of the education system for CWD will be ineffective. In order to achieve this minimum outcome, it will be important to review the SSA systems for identifying children with disabilities entering the education system. In most states, these systems are failing to identify many children with disabilities, and by operating independent systems, may be overburdening anganwadi workers and others with reporting demands. The weakness of identification is in part lack of local capacity, for which there remain major training needs. Improved initial identification needs to be complemented with strengthening of SSA’s simple systems for ongoing school-based assessment of emerging (and often easily reversible) disabilities. However, the broader question relates to pre-school age screening for which MHRD is not responsible, and this is a critical area for further work. All new school construction should be physically accessible and current efforts of retrofitting accelerated. The provisions of the PWD Act to support children with disabilities in reaching school also need more serious attention, ad focusing on the final stages of access is meaningless if children have not been able to access the vicinity of the school.
Improving the quality of education services: GOI should require all states to develop a strategy for delivering education to children with special needs, in order that SSA and other central funds can be allocated in a less mechanical manner. This strategy would assist in improving the currently poor expenditure performance, and more importantly move the system towards a more child-centered allocation which can provide parents and local authorities with more options and greater accountability for resource use. Second, a key element of strategy execution must be making the special needs resource centre model operational. In many states, this will require piloting of different models with good evaluation. Third, current efforts to make the curriculum accessible and adapted to the learning needs of children with disabilities need to be accelerated. For special education curricula, greater efforts to assess the needs of children in activities of daily living and focus learning materials on acquisition of these skills is required. Fourth, as part of this strategy, the Government could also ensure that special education knowledge is imparted to all teachers in pre-service training. Basic training of educational administrators would also be necessary in order to ensure that teachers are encouraged to use their disability-specific skills. In this regard, it would be important to review the performance of Rehabilitation Council of India in its training provision and regulation role.
Strengthening education institutions. This reform would first involve a more direct institutional relationship with MHRD rather than MSJE. Shifting all special education under MHRD, so that planning, financing and monitoring of the education of all children with special needs in the public and aided systems can be done in a coherent manner. Ensuring VECs, CBR groups, womens’ groups, and other community organizations are actively engaged in the importance of educating children with special needs, and familiarized with the benefits for all children educationally and socially will also be important. Finally, as in the case of health service delivery, overcoming weaknesses in public sector implementation by developing public/private partnerships, learning from NGO sector innovations in education of children with special needs, and deepening public/NGO partnerships in those states where they are lagging will be important.
The preceding section focused primarily on SSA/IED as the major public education initiative for CWD. However, education of children with special needs has a long tradition also in the non-government sector, and much of the most innovative work in education for CWD continues to happen outside the public system (or through partnerships where the government finances non-governmental service delivery). This section reviews NGO roles in education of special needs children in India, and assesses the potential for an expanded role for partnerships between government and non-government providers.
As with the government sector, the tradition of NGO education for CWD was one of special schools until at least the mid-1950s. To some extent, this strong tradition continues, both on an independent basis and through the work of NGO special schools funded through the MoJSE NGO grants. In 2003/04, MoJSE provided grants-in-aid to 657 NGOs for a total of Rs. 71 crores and for the benefit of 2.17 lakh people (though this was reduced to Rs. 67 crore in 2004/05). The bulk of this assistance went for residential and non-residential special schools for different categories of CWD. As can be seen, given the numbers of PWD covered by all MoSJE grants, it is clear that the more significant NGO activities are likely to be those carried out independently or as partners/executing agencies within mainstream education initiatives.
Since DPEP and increasingly in SSA, there is a stronger public policy of linking NGO schools for CWD with the mainstream education system, either as direct service providers of different forms, or as resource centres for regular schools. The overall concept of support is to strengthen linkages between general and special educators and educational establishments. The main NGO initiatives which are supported through SSA focus on four main approaches:
- using NGO special schools as resource centres for children with more severe or multiple disabilities who require special therapy or support. This may include provision of services by the special schools on a short term basis to CWD in regular schools, outreach support for mainstream schools to deal more effectively with their disabled students, provision of assessment services, advocacy efforts, and joint leisure and curricular activities.
- involving special schools as demonstration centres for both special educators and regular teachers.
- using special school staff as trainers for teachers in regular schools to strengthen their skills to include CWD in regular settings.
- using special schools to develop learning/resource materials for CWD that will also promote improved learning among all children
- in Assam, NGOs have been tasked with a wide range of services for CWD in 11 districts, with coverage accounting for over 40 percent of all identified CWD in the state under SSA. While the initiative faced challenges in variable capacity of NGOs, successful interventions have been undertaken ranging from identification of CWD, community sensitization, teacher training, resource support to schools, preparation of IEPs, and regular monitoring.
- in AP, there has been a strong push for residential bridge course for CWD aged 9-14 who are out of school. These courses last for 10 months and are intended to graduate CWD into regular schools, and an estimated 3000 CWD were enrolled in such camps in 2005, which is over 2 percent of all identified CWD in the state. While costs exceed SSA standard annual allocations (per child costs for recurrent and non-recurrent costs are around Rs. 4,800), this is less of a concern given low expenditure execution on IED. Other states such as UP also have positive experiences of partnership in bridging courses.
- Tamil Nadu features some of the most innovative and widespread NGO initiatives in education of CWD, with NGO implementing agencies in 391 blocks of the state as of 2005. Their programs include innovative support for home-based education of children with severe disabilities, which includes training of parents and development of skills in the child for carrying out activities of daily living.
- West Bengal represents a well-designed case of trying to establish resource centres at different levels of the education system. The structure is headed by a State Level Resource office operated by 4 experienced NGOs, which performs a coordinating and planning function. This is linked to District level resource Offices in 20 districts, with around 270 special educators in place as resource people. The training function of the DLROs has contributed to West Bengal accounting for around 10 percent of all teachers nationally sensitized in IE under SSA.
It is clear that NGO/government partnerships hold great potential for expanding outreach to and inclusion of CWD in mainstream education. However, more assessment is needed of the extent to which the standardized per child allocations under SSA can accommodate different types of interventions. Even in successful states like TN, there are concerns among NGOs that effective publicly-financed support from NGOs to CWD is being sustained through implicit subsidization from the operations of NGOs themselves. Governments will need to do more work on evaluating the real costs of different modes of inclusive education, as a policy commitment to meeting the individual and special needs of CWD needs to be set against both finite resources and a system of education budgeting which often lacks flexibility.
Even with increased and effective NGO involvement, the primary responsibility for guaranteeing the rights of CWD remain with governments. Increasing the involvement of NGOs needs to avoid the pitfall of education of CWD becoming a “residual” sub-sector. Integrating management of CWD education under the MHRD may be one channel for ensuring that this does not happen. Using NGOs both as advocates and as a source of expertise fore increasing the capacity of mainstream public systems is another key element of such a strategy.
Conclusions and recommendations
More than most areas of policy with regard to people with disabilities, the education sector has been relatively progressive in policy terms. It has also in principle committed to a progressive menu of options for delivering education to children with special needs. However, it is clearly struggling to turn policy into effective practice for a variety of reasons. It seems that there is a major need to get the basics right: identify children with disabilities more effectively; make the content and format of what they learn relevant and accessible; have resources available with adequate outreach to teachers and children; and work through various channels to convince families and communities that educating children with disabilities is worthwhile. However, all this needs strategic direction on inclusive education at state and lower levels of the system which in most states still appears to be lacking to date, though examples such as Gujarat and TN provide guidance on how this can begin to happen. More specific directions include:
Improving identification of children with disabilities and promoting access to schools: This is the absolute priority in the first instance, as without identification and some form of access, any qualitative efforts to improve the inclusiveness of the education system for CWD will be ineffective. In order to achieve this minimum outcome, it will be important to review the SSA systems for identifying children with disabilities entering the education system. In most states, these systems are failing to identify many children with disabilities, and by operating independent systems, may be overburdening anganwadi workers and others with reporting demands. The weakness of identification is in part lack of local capacity, for which there remain major training needs. Improved initial identification needs to be complemented with strengthening of SSA’s simple systems for ongoing school-based assessment of emerging (and often easily reversible) disabilities. However, the broader question relates to pre-school age screening for which MHRD is not responsible, and this is a critical area for further work. All new school construction should be physically accessible and current efforts of retrofitting accelerated. The provisions of the PWD Act to support children with disabilities in reaching school also need more serious attention, ad focusing on the final stages of access is meaningless if children have not been able to access the vicinity of the school.
Improving the quality of education services: GOI should require all states to develop a strategy for delivering education to children with special needs, in order that SSA and other central funds can be allocated in a less mechanical manner. This strategy would assist in improving the currently poor expenditure performance, and more importantly move the system towards a more child-centered allocation which can provide parents and local authorities with more options and greater accountability for resource use. Second, a key element of strategy execution must be making the special needs resource centre model operational. In many states, this will require piloting of different models with good evaluation. Third, current efforts to make the curriculum accessible and adapted to the learning needs of children with disabilities need to be accelerated. For special education curricula, greater efforts to assess the needs of children in activities of daily living and focus learning materials on acquisition of these skills is required. Fourth, as part of this strategy, the Government could also ensure that special education knowledge is imparted to all teachers in pre-service training. Basic training of educational administrators would also be necessary in order to ensure that teachers are encouraged to use their disability-specific skills. In this regard, it would be important to review the performance of Rehabilitation Council of India in its training provision and regulation role.
Strengthening education institutions. This reform would first involve a more direct institutional relationship with MHRD rather than MSJE. Shifting all special education under MHRD, so that planning, financing and monitoring of the education of all children with special needs in the public and aided systems can be done in a coherent manner. Ensuring VECs, CBR groups, womens’ groups, and other community organizations are actively engaged in the importance of educating children with special needs, and familiarized with the benefits for all children educationally and socially will also be important. Finally, as in the case of health service delivery, overcoming weaknesses in public sector implementation by developing public/private partnerships, learning from NGO sector innovations in education of children with special needs, and deepening public/NGO partnerships in those states where they are lagging will be important.