The socio-economic profile of PWD and insights into community attitudes provided in previous chapters suggest that there remain major challenges at several levels in realizing the rights of PWD in India. This chapter explores the policy and institutional framework for promoting full participation of PWD in society. Overall, India has one of the more developed national policy frameworks for disability of developing countries, though there remains scope for improvement, in particular at the sub-national level. However, as in many areas of social policy, challenges of institutional capacity and coordination have contributed to implementation that frequently leaves much to be desired. The intersection of policy and institutions is therefore critical to understanding the factors that drive current outcomes for PWD and might contribute to improving them.
While the primary focus on institutional discussion in the chapter is public institutions, it is clear that non-public actors are particularly important in the disability field relative to other areas of social policy. These include persons with disabilities themselves, NGOs, DPOs, community-based groups such as SHGs or CBR groups, the private sector, and households. While there is a clear need for improvement in the functioning of public institutions dealing with disability, there is equally – perhaps even more importantly – a need for deepening synergies between the public sector and non-public actors, in particular disabled people.
Policies for disability in India
India has a long experience of policy and practice with respect to disability, including collection of census information on disability from as early as 1872, and special schools and institutions operating since the 19th century. Like many countries, it also had specific provision for people with mental illness and retardation under the Indian Lunacy Act of 1912. The Constitution of India acknowledged also general state obligations to PWD in Article 41, and the State List under “Relief of the disabled and unemployable”. Subsequently, specific measures such as employment concessions were introduced from the 1960s. However, it was not until the 1980s that policy commitment to full participation of PWD in Indian society evolved. The outcomes of this policy shift were realized in several key pieces of legislation: (i) the Mental Health Act, 1987; (ii) the Persons with Disabilities (Equal Opportunities, Protection of Rights and Full Participation) Act, 1995 (PWD Act); (iii) the Rehabilitation Council of India Act, 1992 and amended in 2000 (RCI Act); and (iv) the National Trust for Welfare of Persons with Autism, Cerebral Palsy, Mental Retardation and Multiple Disabilities Act, 1999 (National Trust Act). The cornerstone among these is the PWD Act, which is discussed in the following section.
• The Persons with Disabilities Act: The main provisions of the PWD Act are outlined in Box 7.1. It seems clear that the Act is informed by approaches beyond a pure medical model, in that many aspects of PWD lives are addressed, including societal attitudes. At the same time, the direct linkage in the Act between definitions of disability and entitlements necessitates a definition of disability which derives from threshold levels of physical and mental impairment which are defined in a largely medical sense. While the philosophy of the Act therefore represents a major step forward in disability policy in India, its underlying philosophy can be considered a hybrid between medical and social models of disability.
Broadly, the entitlements and commitments towards PWD under the Act can be divided into two main groups: (i) entitlements which are absolute and thus in nature of legal rights. Some of these existed as rights prior to the Act but were reiterated or strengthened in the Act itself (and have in some cases been refined subsequently); and (ii) commitments that are given either in rather general terms or with the explicit proviso “within the limits of [governments’] economic capacity and development”. These can be described as “contingent entitlements” under the Act and are not unqualified rights. The division is not entirely clearcut, as subsequent jurisprudence has in some cases strengthened general commitments. In a number of cases, follow-up action is also anticipated by states or other relevant authorities.
Despite the PWD Act being a ground-breaking piece of legislation, there remain a number of policy shortcomings in its design that are worth highlighting. These include both general issues which apply to several areas of the Act, and others which relate to specific sectoral heads. A number of them were raised by GoI’s own Amendment Committee in 1999, but have not subsequently found their way onto GoI’s agenda.
General Policy Issues in PWD Act: Some of the cross-cutting policy issues with respect to the PWD Act include:
•the Act covers only designated groups of PWD, which is by no means completely inclusive of categories of disability. This is in part driven by the linkage in the Act between the relevant legal definition of disability and the entitlements under the Act that flow from that. There is a natural reluctance on the part of policymakers to commit to entitlements for a wide group in the face of limited financial and other resources. Nonetheless, there is no reason in principle why the definitional and entitlement aspects of the Act need be completely synchronized. Providing for a more inclusive definition of disability while retaining more restrictive entitlements by disability type has been proposed by the Amendment Committee for the PWD Act. 6 The Committee proposed expansion of the Act’s definition of disabilities to include multiple disability, autism, thalassemia, haemophilia, filiariasis, cerebral palsy and moderate/severe speech impairment. It also provided a more precise definition of mental illness, which in the current Act is vaguely defined as “any mental disorder other than mental retardation”. These proposals seem eminently sensible. On the latter point, amendments to the Act proposed by the Ministry in 2006 also represent a step forward in trying to have a more workable definition of mental illness.
a second overarching policy issue with the Act relates to commitments which are subject to the “limits of economic capacity and development” of the relevant authorities. The formulation represents an attempt to balance policy commitments and fiscal and institutional realities. While the approach is reasonable, the Act fails to outline any process for determining broadly what are the appropriate levels of policies and interventions which might be expected at different levels of economic development within India. This could not, of course, be a very precise process, but without some indication of what are reasonable expectations of states at different levels of economic development, it is difficult to know what constitutes reasonable compliance effort on the part of the authorities. As a result, what are justiciable rights in sections where this proviso is used remains quite uncertain. The uncertainty is significant, as this approach is used in important sections such as identification of PWD, prevention and treatment of disability, and access rights of PWD.
In the absence of a process for benchmarking reasonable performance by states on the contingent entitlements of the Act, the courts have become the main point of reference for PWD to enforce performance by governments. In this respect, the courts have sought to promote the rights of PWD in a variety of areas. The courts have tried to balance PWD entitlements with fiscal concerns. However, the resources and time needed to access the courts effectively are significant, and are likely to exclude many PWD.
•the above point raises the wider one that the Act’s entitlements and commitments are supported by a weak enforcement mechanism. The institution mandated with monitoring compliance with the Act – the Office of the Commissioner – has weak powers. The Commissioners’ office has authority to look into deprivation of PWD rights and on-implementation of various rules, laws etc. which have been developed to promote the welfare and rights of PWD. The fundamental limitation of the office is that its only legal sanction in case of a breach is to “take up the matter with the appropriate authorities”. The Office does not itself have enforcement powers of a court or administrative tribunal. It can and does make orders, but can not enforce compliance. As such, its effective powers are either “naming and shaming” or encouraging referral to the court system. While these have been effective remedies in some cases, there are clear limitations. This issue is discussed in the institutions section.
• the overall approach of the Act has rather limited roles for actors outside the core administrative framework, including NGOs/DPOs, civil society, PWD themselves and PRIs. There is no explicit role for PRIs mentioned, though the Act was passed after the 73rd Constitutional amendment. With respect to the NGO sector, it is mentioned at several points as either a point of consultation (e.g. on formulation of PWD rehabilitation policies) or as a potential implementer (e.g. on disability research and training of teachers). However, the overall policy and delivery model remains a rather traditional administratively-driven mechanism, with limited sense of genuine partnership in policy development and service delivery between the public and non-public sectors. Perhaps most notable of all is that DPOs are not mentioned in the Act at all, nor any obligation for governments to consult directly with PWD when developing policies, designing interventions or monitoring performance. The assumption of the Act appears to be that disability NGOs will act as conduits for PWD views and action.
Sectoral policy issues in the Act: There are also several sector-specific policy issues worth noting. They include:
•Employment: With respect to public sector employment, the Act provides for 3 percent of “identified posts” to be filled by PWD. The current list of posts (identified only in 2001) is restrictive, arbitrary and based purely on impairment, without consideration of personal or environmental factors. There are also no sanctions for non-compliance. This is discussed further in Chapter 6. The overall approach is one that is not considered good practice internationally, even in systems where a quota approach is used. A second feature of the quota policy is that it applies only to three disability types – locomotor, visual and hearing, with a 1 percent reservation for each. Thus even the full disability categories of the Act are not included in the reservation policy.
•Education: While the thrust of the Act to ensure that CWD are in school is clear, its guidance on the most appropriate type of education and who should take the decisions on that issue is less so. The Act provides that education of CWD should be in “an appropriate environment”. However, it has a multiple track of promoting integration of CWD into regular schools, setting up of special schools, and home-based education. While the different approaches need not be contradictory, the Act provides limited guidance both on which approach should be considered preferable and on who is to take and enforce decisions on what is considered an appropriate educational environment for individual children. Subsequent policies have provided some more guidance on the issue, but whether it remains the right of parents where to school their children is unclear.
•Health: Apart from being subject to the economic capacity proviso, the provisions of the Act in the area of health are very limited. Perhaps the most notable point is that the obligations of the authorities are so generally phrased that they are difficult to interpret in terms of enforcement. Thus, the authorities should pursue “various methods for preventing disabilities”, “take measures” for promoting pre-, peri- and post-natal care, and “create awareness” of disability issues. The combination of the economic capacity proviso and such general language makes it difficult to consider the provisions on prevention and early detection of disabilities as more than statements of intent. The fact that the subsequent jurisprudence on health issues relates almost entirely to issues of custodial treatment of mental health patients and their capacity in personal law seems to support this conclusion.
As of 2006, the Ministry has proposed a number of amendments to the PWD Act which are under consultation. The general areas for proposed revision are:
•revision of definitions of a number of disabilities, including mental illness, cerebral palsy, low vision, mental retardation and other impairments. For several of the conditions, a positive element of the proposals is that they take into account more explicitly the impacts of impairments on functions and activities of daily living. On the other hand, there is a question as to whether the Act itself is the most appropriate place for precise medical and other definitions of disabilities, or whether the implementing Rules may give more flexibility in adjusting definitions over time.
•and oversight of the Act. Some of this is (appropriately) moving precise definition of institutional composition and other details into the implementing Rules. Others make the mandate of bodies such as the central Coordination Committee more general and overarching in nature.
| Box 7.1: Key entitlements and commitments under the PWD Act, 1995 | |
| The PWD Act has both binding entitlements and more general commitments. The key provisions are: Education: The following are binding on Government (i.e. not subject to economic factors): • Governments shall ensure that every CWD has access to free education “in an appropriate environment” until the age of eighteen. •Governments “shall initiate or cause to be initiated” research by public and non-governmental agencies for development of both assistive devices and special learning materials for CWD in order to promote equal opportunity in education. •Governments shall ensure teacher training that produces “the requisite manpower” for teaching of CWD both in special schools and integrated settings. •all public educational institutions and other receiving aid from Government shall reserved not less than 3 percent of seats for PWD (i.e. for PWD over 18 years). •government should prepare a “comprehensive education scheme” for CWD which includes transport or financial incentives, barrier free access, supply of book, uniforms and learning materials to CWD, adjusts the examination system as necessary, adapts curriculum for CWD. Employment: The Government shall: •identify posts for PWD in public establishments and update the list every three years. •reserve not less than 3 percent of identified posts for PWD, with 1 percentage point reserved for people with blindness/low vision, hearing impairment, locomotor disability or cerebral palsy respectively (though any department or establishment can be exempted by notification). •every employer should have a record of all PWD employed in that establishment. •Governments and local authorities shall formulate schemes for promotion of employment of PWD which may provide for training of PWD, relaxation of age limits in employment, measures related to OHS, provisions for financing such schemes etc. •Reservation of not less than 3 percent in all poverty alleviation schemes. •“within the limits of their economic capacity and development”, Governments shall provide incentives to both public and private sectors for employment of PWD with a target of at least 5 percent of their workforce to be PWD. Prevention and early detection of disabilities: All commitments in this area are given with the proviso “within the limits of their economic capacity and development”. With proviso, Governments should: •Undertake surveys on causes of disability. •Promote “various methods” for preventing disabilities. •Screen children at least once a year for identifying at-risk cases. •Provide facilities for training PHC staff. •Conduct or sponsor awareness campaigns on hygiene, health and sanitation, and on causes and prevention of disabilities. •“take measures” for pre-, peri- and post-natal care of mother and child. Affirmative Action: Governments shall frame schemes for: •Provision of aids and appliances to PWD •Preferential allotment of land for housing, business, recreation centres, special schools, research centres, and factories run by PWD entrepreneurs. Non-discrimination in access: All commitments in this area are given with the proviso “within the limits of their economic capacity and development”. With proviso, Governments should: •Adapt all forms of transport to make them accessible to PWD. •Provide for a variety of assistive devices in the built environment, including auditory signals, ramps in public buildings and health facilities, Braille signage, accessible curbing, marked zebra and railway crossings, warning signals as appropriate etc. |
•in the area of education, the proposed revisions aim to give a more specific obligation to states and local authorities to develop IE strategies and schemes. This increases consistency with initiatives under the lead of MHRD.
•other sectors such as employment attempt to spell out more precise obligations of employers and mandates of institutions. However, it is not clear how the proposed revisions will result in more effective functioning of actors such as Special Employment Exchanges.
•strengthened provisions on regular gathering of data on the socio-economic status of PWD.
Implementation of the Act: Previous chapters discuss in detail outcomes to date in implementation of the PWD Act. A generic policy question however is the extent to which states or other relevant authorities have met their commitments under the PWD Act to frame state-specific entitlements or schemes. As could be expected, the relative performance of states in this regard exhibits major variations, with some states quite active in framing schemes and trying to strengthen institutions, while others have to a large extent ignored their obligations under the Act for follow-up measures. GoI’s most recent assessment of performance at central and state level indicates that overall implementation performance has been poor, and in a number of areas very poor, with an overall evaluation that the “act is being poorly implemented” eight years after its enactment.
There are a range of institutional reasons which contribute to this outcome and are discussed below. However, there also appears to be more basic questions of relative political commitment between states. Better performance has not simply been a case of better-off versus poorer states, or high versus low capacity states. Some poor states (e.g. Chhattisgarh) have made serious efforts to elaborate their policy commitments. However, CAG in 2004 identified a number of states in most areas of the Act which had taken no action to fulfill their obligations as of end-2003. These include prevention and early detection of disabilities (where even large states such as Maharashtra, West Bengal, Jharkhand and HP had taken no action in the 8 years following the Act), several elements of education, employment (where several states had failed to identify any posts for PWD), affirmative action, and provision to promote access of PWD.
•Awareness of the PWD Act: A key ingredient of effective implementation is awareness. A decade after this landmark legislation, what is the level of awareness of both the Act and specific entitlements under it ? Recent survey evidence from villages in TN and UP gives some insights. Overall, awareness of the PWD Act in the states studied remains very low, and lower among households with PWDs than those without them. This is shown in Table 7.1. Only around 4 and 7 percent of PWD HHs in UP and TN respectively were at all aware of the Act, and around 8 and 9 percent of non-PWD households. Among those who were at all aware of the Act, the share who were very familiar with the Act was also low, particularly among PWD households.
| Table 7.1: Awareness of the PWD Act is very low and lower among PWD households than others | ||||
| UP PWD HH | UP non-PWD HH | TN PWD HH | TN non-PWD HH | |
| Aware | 4.1% | 7.5% | 6.8% | 8.9% |
| o/w very familiar | 6.3% | 26.1% | 7.4% | 11.1% |
| Not Aware | 95.9% | 92.5% | 93.2% | 91.1% |
The survey also asked about awareness of specific entitlements under the Act. While awareness of specific entitlements was significantly higher than of the Act itself, it remained low for most benefits, with well less than half of PWD households aware of entitlements. (Figure 7.1) A second important observation is that awareness was substantially higher in TN than UP, and for some entitlements such as disability certificates and subsidized credit. Perhaps the most striking finding is that over 80 percent of PWD households in UP were not aware of the process of certification as a PWD, which is the key threshold requirement for access to nearly all others. 11 However, the TN findings (and work in Gujarat) suggest that there is considerable variation across states on the issue, with the relative strength of civil society and NGOs important.
Awareness of entitlements under PWD Act is also low, though with strong state variation

The above findings are supported by evidence from states such as Orissa which have also found low awareness of the PWD Act entitlements among a range of civil society and public sector actors. The findings point not only to a general need for raising awareness of the rights of PWD (and suggest that greater reliance on non-governmental channels of information dissemination may be worth considering), but also the need for more focused information outreach to the core target group of PWD households themselves.
Recent developments in disability policy:
National Policy on PWD: In 2005, the MoSJE developed a draft National Policy for Persons with Disabilities. This was approved by the national Cabinet in February 2006 and is available on the Ministry website. Overall, the Policy follows the structure of the PWD Act. Several observations can be made:
•the policy represents progress in policy terms on some shortcomings of the PWD Act. These include: (i) greater recognition of the role of NGOs and CBOs in service delivery and policy for PWD, including the need for more consolidated information on NGO activities, increased efforts to address regional imbalances in disability NGO coverage, etc; (ii) a more elaborated approach to education of CWD (though the core issue of who decides where a CWD does to school remains unclear); (iii) a clearer acknowledgement of the role of media in awareness raising about disability issues; and (iv) acknowledgement of significant issues in collection of statistics on PWD (though the draft offers no strategy for how disability statistics can be improved).
•the Policy often repeats general commitments of the PWD Act, though remains more general on concrete strategies for implementing them. This major shortcoming is not for want of insight into the shortcomings of current policy and practice. For example, the POlicy sets out succinctly the reasons why the current disability certification process has not functioned well. However, in terms of the forward-looking agenda, its merely urges state Governments to adopt “simple, transparent and client-friendly procedures”. There is no strategy for how the situation might be improved. This is one example, but such lack of concrete strategies is found in many parts of the document. This is not true in all areas (e.g. health strategies are outlined in somewhat more detail). However, overall there is very limited sense in the Policy that even GoI’s own assessments indicate serious implementation problems. Simply reiterating the general commitments of the PWD Act is unlikely to be sufficient to reinvigorate the disability sector.
•there remains limited reference to the role of PWD themselves in policy development, implementation and monitoring and evaluation. DPOs are not mentioned in the Policy, nor are PWD themselves. Rather, they remain agents who interact with the public policy and delivery systems either through public agencies or at best NGOs. While the Policy notes that “PWD are an important resource for the country, and seeks to create an environment that provides them with equal opportunities, protection of their rights and full participation in society”, this critical insight is not reflected in the main Policy.
•there remains no strategy for integrating disability concerns into the work of PRIs. While the importance of PRIs is acknowledged, this remains an under-developed element of the Policy given the increased importance of PRIs in many areas of service delivery.
Education policy: An important point to note at the national level is that policy has progressed significantly in some areas since the PWD Act. In particular, in the area of education, policy towards inclusion of CWD into mainstream education has become increasingly clear in recent years, and the policy statement of the MHRD in 2005 represents a more robust and concrete commitment to realizing the right to education of CWD. This is discussed in detail in Chapter 4.
State policies on disability: An additional aspect of disability policy that has remained relatively neglected is development of state-level disability policies. To date, the only states that have draft disability policies are Chhattisgarh and Karnataka, though Maharashtra has a state level Action Plan for implementing its commitments to PWD. The draft Karnataka policy for the most part mirrors the structure and major provisions of the PWD Act. For the most part, it is a state-specific endorsement of various initiatives for promotion of rights of PWD. In a number of cases, it repeats the PWD Act entitlements and commitments, and repeats general instructions to frame relevant schemes (e.g. reservation in poverty alleviation programmes; education). In others, the general commitments of the Act are put in a more state-specific context (e.g. health). In still others, there is more specific guidance on circumstances in which PWD should avail commitments under the Act (e.g. exemptions on property tax for PWD). For the most part, however, the draft state policy does not provide much more specific commitments or implementation guidance than the Act itself.
In contrast, the Chhattisgarh draft state policy – the Comprehensive Disability Policy Framework for Chhattisgarh – can be considered “best practice” within India, and could provide a model for future national and state-level policy development. The Policy provides more thorough context and strategic direction for disability policy, allowing for greater prioritization in planning and implementation. The Chhattisgarh policy is outlined in Box 7.2, and in 2007 was approved by the state Cabinet, and will be submitted to the Assembly.
| Box 7.2: Good Practice in State-level Disability Policy-The case of Chhattisgarh | |
| Despite being a poor and new state, Chhattisgarh has developed an impressive draft state level policy on disability – the Comprehensive Disability Policy Framework. Overall, the draft Chhattisgarh Policy provides useful guidance for other states in policy development. Some important features are: •it has explicit discussion of different models of disability and frames policy accordingly •it acknowledges India’s international obligations in the area of disability policy •it has clear statements of both overall and sectoral policy objectives, indicating the overall policy stance on all major issues •at the next level, it provides guiding principles in aiming reach policy objectives •it acknowledges that “self-representation” of PWD in disability policy and practice is critical •it identifies special cross-cutting areas in need of special attention, including mental illness, gender issues, and prevention and early detection of disabilities •it establishes a State Disability Council as an institutional means both of raising the profile of disability issues and improving coordination •it sets specific coverage/performance targets by sector, thus moving towards monitorable indicators of progress •it is explicit on strategies to mobilize public financing for the sector. |
UN Convention: As of March 2007, India is a signatory of the UN Convention on the Rights of Persons with Disabilities. The Convention is a milestone in the priority accorded by UN members to disability, and GoI is undertaking consultations during 2007 to familiarize stakeholders on its implications for India. While further consultation is needed, some areas where the Convention is likely to have implications for disability policy in India include: (i) a wider definition of “accessibility”, going beyond the physical environment which is the focus of current access policies (e.g. access to information); (ii) greater focus on what “economic capacity of states” means in practical terms; and (iii) expansion of the definition of disabilities to include some areas like developmental disorders which are not covered under the current Act.
Conclusion: Despite its many positive features, there is scope for improvement in the policy framework for disability in India, particularly at state level where policy development has been largely piecemeal. The more fundamental issue is the extent to which the entitlements under the Act have been realized in the decade since its passage. The issue that the rest of this chapter addresses is institutional mechanisms which the Act had put in place to enforce entitlements and increase accountability of providers, and how effective have they been in practice.
Institutional Issues in Implementing Disability Policies
Given the diverse range of issues that PWD deal with, it is not surprising that there are major challenges of institutional coordination in disability policy. These are between levels of the public sector (e.g. centre/state/districts and lower), within levels of the public sector (e.g. between social welfare, health, transport, education, and labor departments), and between the public and non-public sectors at all levels of the system. While this section focuses primarily on more formal institutions in disability policy and service delivery (both public and non-public), it is also important to stress the importance of informal institutions – the most important by far being families with disabled members. Given market and government failures, the family remains by far the most important institution in the lives of PWD in India.
•The formal institutional framework for disability: There is a complex institutional framework for operation of the disability sector in India (see Figure 7.2). The nodal agency for disability is the Ministry of Social Justice and Empowerment (MSJE), whose overall mandate is to promote the interests of “disadvantaged and marginalised sections of society”. This includes Scheduled Castes, Backward Classes, minorities, PWD, aged persons, street children, victims of drug abuse, and others. There are inherent challenges for any nodal ministry in such a multi-sectoral field as disability. To that extent, there is no “natural” nodal Ministry for disability issues as there may be in sectors such as education or telecommunications. That said, there are areas where having MSJE as lead agency seems questionable and out of line with better international practice. The primary example is special education. Presently, this is under the mandate of MJSE, as are in-service training initiatives for teaching of children with special needs through RCI (which is administratively under MJSE). The consequence of this is that the vast majority of CWD have their education under the mandate of MHRD while those in special schools are under another Ministry. There does not appear to be a good rationale for this other than institutional inheritance. Equally, better practice internationally is to have education of all children under educational authorities (see Chapter 4 for further discussion).
In the period 1998-2003, just under Rs. 1042 crore was spent by MSJE on the” welfare of PWD”, with the largest expenditure category the national institutions and corporations for disability, support to NGOs in service delivery to PWD, and spending on aids and appliances. This represents a negligible portion of total budgetary spending. While precise comparisons are difficult, for 2000-2001 budget year, MJSE’s spending on disability would account for around 0.07 percent of total GoI expenditure, and for 2002-03, it accounted for around 0.05 percent of total. In the most recent budget year (2005-06), the share had fallen even further to only 0.047 percent of total allocation. Interestingly, the nominal allocation for 2005-06 was lower than for either 2000-01 or 2001-02. Such spending figures indicate the low priority placed by GoI on its core programs for PWD. While spending under other ministries may have risen in some cases (e.g. education, where spending on IE under SSA has increased significantly in recent years), unfortunately, MJSE do not have consolidated figures on a cross-ministerial basis for spending on PWD by other ministries, so that it is not possible to have an aggregate picture
Apart from specific sub-sectors where the nodal function of MSJE appears to be of questionable value, there is a broader challenge of “convening power” for a Ministry which is overall a low spending agency relative to several ministries which it must coordinate (in particular, education, health, transport and public works). Again, there is no ideal solution to such an issue, but what it points towards is the unusual importance in disability of inter-sectoral institutional coordinating mechanisms.
Figure 7.2: Governmental Structure for Policy and Implementation of Programs for the Disabled in India
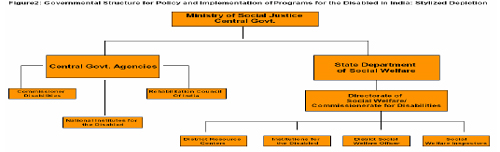
To address the concern of inter-sectoral coordination, the PWD Act mandates central and state-level Coordination and Executive Committees (the latter intended as the executing arm of the former). Together, these Committees are intended as “focal points on disability matters” and to be key institutions in development of comprehensive disability policy development. They should meet every 6 and 3 months for the Coordination and Executive Committees respectively. Unfortunately, the track record of these coordinating institutions in states and at the centre is poor, with few exceptions. GoI reports indicate that meetings in most states happen very rarely, with a number of major states (e.g. Gujarat, Bihar, Kerala) having had only one meeting of their Coordination Committees since the passage of the Act, and others such as Rajasthan and Orissa reporting no meetings at all. Similar lack of action seems to apply to State Executive Committees. CAG found that the shortfall in meetings of these core committees as of end-2003 was between 43 and 100 percent at state level and 50 percent at the national level. It is unclear if the situation has improved in the meantime. It thus appears that the disability field is characterized by a nodal Ministry with relatively weak convening power, and coordinating institutions which are in many parts of the country barely functional.
The above situation makes the role of the Commissioner for Persons with Disabilities (CPWD) even more crucial. The PWD Act mandates an Office of the Commissioner for Persons with Disabilities, with the Chief Commissioner at national level and State level Commissioners’ offices in all states. It is tasked as the primary public institution with respect to regular oversight of the Act – the “watchdog” for the disability sector. These offices are mandated to coordinate the work of various agencies, to monitor fund utilization on disability programs, and “take steps to safeguard the rights and facilities made available to PWD”. An important element of the last function is the grievance mechanism of the Commissioners’ offices, which have a quasi-judicial complaints and hearing mechanism.
An area where the Chief CPWD Office has, given its staffing and other resource limitations, improved performance in recent years is grievance redressal. The number of settled cases through its quasi-judicial process has increased markedly in recent years, rising from 718 settled claims in 2003-04 to 1,333 in 2005-06. The proportion of pending cases in total registered has also fallen. Of total cases in recent years, around half were initiated suo moto by the CPWD office itself, though this proportion is falling, perhaps reflecting greater awareness of its grievance redressal functions. Of cases registered in 2004-05, over half were employment related (both hiring and issues of transfers, promotions etc), with the remainder spread thinly across benefit issues, harassment claims, education and other matters.
There is little detailed analysis of the performance of the Commissioner system outside its own reports. However, the most recent GoI report suggests significant issues of low capacity to perform their mandate effectively. CAG evidence for the period 1999-2003 indicates several concerns related to: (i) poor monitoring of use of funds; (ii) lack of clarity on grievance redressal mechanisms; and (iii) limited advocacy work in a number of states. The analysis points to significant issues with lack of staff and low capacity in Commissioners’ offices. These concerns are supported by field work for this report in Rajasthan and Karnataka (two states considered to have better functioning offices), which found skeletal staff in both offices. In Rajasthan, the Commissioners’ office consisted of one Additional Commissioner (there has been no Commissioner since end-2003) and his PA, with no support staff. The office had failed to register any grievance cases of PWD since 2002. The same study also noted that full time Commissioners exist to date only in a minority of states. An additional generic concern is the lack of legal expertise in the Commissioners’ offices, particularly at state level, despite the importance of their quasi-judicial role in enforcement of the Act.
Beneath the state level, the nodal function in disability tends to be an additional charge for District or Additional Collectors and BDOs. These act as initial points of grievance redressal for PWD. Apart from these additional charges, states vary significantly in whether or not dedicated staff exist at lower levels who are specifically dedicated to PWD issues. For example, in Karnataka, there are District Disability Welfare Officers, while these are not present in Rajasthan. Essentially, dedicated official functionaries cease at best at district level, below which additional charges are the mode of oversight and service delivery.
Karnataka has been one of the more active commissioners’ offices, and has piloted a number of initiatives, for which is has been recognized as the model state for implementation of the PWD Act. This is despite the office being subject to similar resource constraints as many others. The distinctive feature of the Commissioners’ office in Karnataka is that is has carved out a role which is somewhat independent of the state Social Welfare Department. Some of the innovative features of the operation of the Karnataka office are presented in Box 7.3.
A further significant institution in the disability field is the National Trust For Persons with Autism, Cerebral Palsy, Mental Retardation and Multiple Disability. Its objectives are to: (i) enable and empower persons with disability to live as independently and as fully as possible within and as close to the community to which they belong; (ii) strengthen facilities to provide support to persons with disability to live within their own families; (iii) extend support to registered organizations to provide need based services during the period of crisis in the family of persons with disability; (iv) deal with problems of persons with disability who do not have family support; (v) promote measures for the care and protection of persons with disability in the event of death of their parent or guardian, including evolving. •The missing pieces – PRIs and disability: As noted in the policy section above, PRIs are largely absent in public sector disability policy and practice. This results in an institutional framework for disability which is increasingly out of line with the constitutionally-mandated developments in decentralization of service delivery and oversight. The relative lack of attention to PRIs continues in the National Policy. In addition, the field work in rural UP and TN for this report revealed that panchayat officials were generally just as ignorant as the rest of the community, not only on the entitlements of PWD, but also in terms of knowledge about causes of disability and attitudes to PWD. An important initial step of an institutional strategy for integrating PRIs into the disability institutional framework would thus be including disability sensitization in the general training courses which PRI officials will undertake in coming years. Efforts by the NGO sector to sensitize village officials have show positive results in rural Rajasthan (see para. 35). This would be particularly important at the gram panchayat level, given evidence of public sector institutional shortcomings in the disability field as one moves further down the system. While GPs will have many issues of weak capacity for some time to come, current evidence suggests that existing institutional arrangements for disability are largely ineffective at the village level, and that new approaches are needed.
| Innovations in Karnataka by the Disability Commissioner’s Office | |
| The Karnataka Commissioner for Disabilities has introduced several progressive practices. These include: •District Disability Management Reviews (DDMRs): This involves regular reviews at state and district levels of all schemes which are targeted to PWD. The process is intended to identify gaps/shortcomings in policy, program coverage, and implementation. Quarterly reports are solicited from relevant departments in specialized format and the results publicized in the media. Collection of information is facilitated by a District Disability Welfare Officer. While reporting is timely, there remain concerns about the reliability of information from line agencies. •Lok adalats for disability: The Commissioner’s office has organized periodic lok adalats (peoples’ courts) in districts for PWD to air their grievances with respect to entitlements. The adalats are chaired by a senior official of the Commissioners’ office. All district officials – including Collectors and officials from social welfare, education, health PRI and other departments – are expected to be present. The process has in some cases led to immediate resolution of PWD issues, or in others accelerated judicial intervention. •Partnerships with voluntary organizations: The Office has actively pursued partnerships with VOs to overcome its capacity constraints. For example, the Alternative Law Forum in Bangalore offers free legal aid to PWD through the Office. This not only includes issues with respect to PWD Act entitlements, but broader issues of access of justice for PWD. •Active use of media: The Office has been one of the most active in raising awareness of disability issues, and in using media to reach its PWD constituency. This includes publicity about violations of PWD rights. Apart from print media, the Commissioners’ office has regular phone-in programmes, which have involved people from throughout the state in direct phones to officials of the Office. |
Source: Bhambani (2006).
• PWD access to public institutions: Very little empirical evidence exists of the interactions of PWD with the official institutional network. This issue is discussed in detail in sectoral chapters which follow. However, the UP and TN survey asked questions on PWD interaction with the public administration and delivery network, and the results provide insights on institutional constraints to access to services and entitlements. Several findings emerge:
• reflecting the limited downward reach of the disability institutional network, the institutions from which PWD most often reported receiving services and benefits were at district level, though panchayats were growing in significance. Results are shown in Table 7.2.
• a substantial share of PWD report difficulties in receiving disability benefits and services. Around 43 percent of respondents indicated that they had not received any benefits or services, with a further 20 percent reporting receiving only some of their benefits or services.
| Table 7.2: Institutions providing benefits and services to PWD in rural UP and TN, 2005 | |
| Panchayat office | Share of those accessing services reporting (multiple answers possible) |
| PHC | 6.7% |
| District or other hospital | 45.7% |
| BDO | 21.6% |
| District welfare office | 38.5% |
| District disability official | 19.7% |
| District Chief Medical officer | 15.9% |
| State welfare or disability official | 4.4% |
| Other | 9.1% |
Source: UP and TN village survey. Bank staff estimates.
• in terms of the major difficulties faced in applying for disability-specific benefits, a range of factors were at play. Close to 30 percent of PWD reported no difficulties in accessing services/benefits. Among the over 70 percent who did report difficulties, three broad groups of difficulties emerge: (i) physical access problems, due to distance, lack of transport or physical barriers; (ii) problems with procedures and/or officials administering the system; and (iii) communication difficulties. The results are shown in Figure 7.3.
| Figure 7.3: Top Difficulties in Applying for PWD benefits and services, UP and TN, 2005 |
 |
While the above results are from two states only, they are consistent with field findings in Rajasthan and Karnataka, and with a variety of studies on PWD access to services. Together with the generally low awareness of entitlements, they suggest that public institutions need to develop far more effective outreach strategies if PWD are effectively to access their entitlements. An obvious area for policymakers to consider is how the PRI system can be mobilized in such outreach, given that only one fifth of current PWD beneficiaries are using that channel to access services. A second issue is how the public sector can more effectively partner with the non-governmental sector and civil society to achieve greater grassroots penetration of awareness and access to services. The following section looks at the role of the NGO sector in the disability field.
The NGO sector and disability: In light of the major challenges in the effectiveness of public sector institutions for PWD, non-governmental institutions assume unusual significance. The role of NGOs is also important to consider in light of the relative obligations of the state and civil society, with a number of practitioners in India seeing an over-reliance on NGOs in the disability sector. A positive feature of the 2006 National Policy is that it gives very clear recognition of the role of NGOs in service delivery, and encourages their greater future involvement in policy development and other areas.
NGOs working in the field of disability are indispensable to supplement and support the efforts of the state in cases where the market fails to be a reliable or accessible source of services. As one would expect, disability NGOs divide along several lines:
• place of operation. There is a strong urban bias in disability NGO presence and activities. There is also a strong state-wise concentration of disability NGOs, with a generally stronger presence in southern states. In addition, states where NGOs are very active are not necessarily ones with a concentration of disability NGOs (e.g. Rajasthan).
• area of focus. While there has traditionally been a strong focus on education and rehabilitation activities, a wider range of issues are being taken up by disability NGOs (e.g. access to justice; participation in voting). This reflects to some extent a difference between disability NGOs with a service delivery focus and those with an advocacy focus.
• philosophical tradition: As in the NGO movement more broadly, disability NGOs reflect a variety of traditions, including Gandhian, Christian, Secular, Hindu, and Muslim. In some sectors, some traditions have had strong presence (e.g. Christians in special education).
• the large majority of disability NGOs have been on a disability-specific basis, with cross-disability NGOs and networks only emerging in the last decade. To date, there has been a higher share of NGOs providing services for the blind and hearing impaired than for persons with locomotor disabilities and mental retardation. NGOs dealing specifically with mental illness continue to be very limited. One result of the disability-specific focus of NGOs has been that until recently the sector often did not speak with one voice. However, Tamil Nadu shows that this fragmented tradition is being overcome in some states.
A recent sample survey of the non-profit sector in India puts the total number of NGOs at 1.2 million. They employ nearly 19.4 million persons, many of whom work on a voluntary basis. There are no comprehensive statistics on the numbers of NGOs that work in the disability sector, but the numbers of organizations known to be working in disability has increased. Data from the mid-1990s suggest that there were more than 2000 NGOs working in the area of disability. More recently, the Delhi DRC reports 5,231 such NGOs. It is not possible to identify the number of organizations working with different types of disabilities.
According to MSJE, in 2003-2004, grant-in-aid funds of just over Rs. 71 crore were provided to 657 voluntary organizations and benefited 217,000 PWD. During 2004-05, the amount was reduced to Rs.67 crores for 700 voluntary organizations. The majority of funds were allocated to residential and non-residential schools for different categories of disabilities. There were distinct differences in government allocations to NGOs between states, which are not systematically related to the number of PWD in the state or their share in the national total PWD population. 28 There is a need to look at how funds can be allocated across states to ensure greater equity in NGO and PWD coverage. In addition, NGOS addressing disability issues appear less reliant on government funding when compared to the entire non-profit sector in India, with an estimated one quarter of disability NGO funding from Government and around 32.4 percent of general NGO revenues from Government funding.
| Box 7.4: Disability For a in Tamil Nadu | |
| There is evidence of good collaboration amongst NGOS and between NGOS and the state in Tamil Nadu: Vellore District Disability Network: 12 disability related organizations meet quarterly to share resources for the rehabilitation of persons with disabilities. The District Disability Rehabilitation Officer is present and occasionally the Disability Commissioner Disability Forum: A disability forum of 23 NGOs (disability specific and development) is facilitated by the Organisation for Development Action (ODA). This forum shares information, knowledge and refers between NGOs. There is reluctance by some organizations in this forum to lobby for change as they receive government support and were concerned about what impact their involvement may have on access to state resources. Hence issues identified in this forum are used for lobbying the government directly by ODA and other interested parties. In August 2005, a State Resource Training Centre for PWD was set up in Chennai under the National Programme for Rehabilitation of Persons with Disabilities (NPRPD). Different NGOs with disability specific expertise are providing their voluntary services for training of persons with disabilities. The centre will showcase good NGOS practices. A weekly radio programme call Thiramaiyin Thisayil (In the Direction of Your Abilities) is broadcast by Ability Foundation in association with all-India radio. It focuses on issues and policies which affect the rights of PWD. Other NGOs also use the show as a vehicle for spreading information on vocational training programmes, and to publicize events such as job fairs. Letters and responses from remote rural towns of TN indicate significant penetration. Source: Officer (2005). |
Disability NGOs operate with many different methods and goals and hence with diverse actors. Examples of interactions among NGOs and between NGOs and the public sector in Tamil Nadu are presented in Box 7.4. It is not possible to characterize these patterns of interaction in a comprehensive manner, but general patterns can be seen, including:
•links between the Government and the non-government sectors. Many NGOs have links with public agencies, predominantly for direct contracting out of services, technical assistance and training. A common source of interaction is with RCI, with NGOs operating special educators’ courses for teachers, though numerous other examples exist in the fields of vocational training and rehabilitation. While results have in many cases been positive, there remain concerns about weak monitoring of NGO performance and hence accountability for use of public funds. However, very few NGOs have had direct influence on disability policy development. There are certain key forums to which select NGOS are invited, e.g. five NGOs working with different disability groups are also involved in each of the central and state co-ordination and executive committees. However, for the most part consultation between the public and NGO sector on disability policy issues remains under-developed, both at the centre and in most states. In addition, NGOs in some cases are acting as watchdogs of the public sector delivery mechanism, as examples such as VSS in Rajasthan and their oversight of the disability certification process attest. The monitoring and evaluation role for NGOs seems one that could more explicitly be developed within public interventions, provided that conflicts of interest in service delivery and monitoring can be minimized.
•interactions between disability NGOs and DPOs are for the most part absent in the states reviewed for this report. This remains an area in need of development for the NGO sector as it is for the public sector, with many NGOs still speaking for PWD. DPOS or PWD-led NGOS should be key collaborators in the design, monitoring and evaluating of training and employment projects and strategies. This is not necessarily simple, as DPOs will frequently require capacity building to engage both with NGOs and with public sector actors. In this respect, CBR is in some states a promising vehicle to act as a bridge between DPOs and other actors in the disability field. Equally, states such as AP and Karnataka have good experience with creation and empowerment of PWD SHGs in their broader rural development initiatives.
•there are indications of growing collaboration between disability NGOs and development organizations to identify and support in economic rehabilitation PWD in remote rural areas. While many of these initiatives are highly localized, larger projects such as DFID’s Poorest Areas Civil Society Programme, and World Bank supported efforts in AP (and more recently TN) suggest that there is potential for such collaborations to achieve significant scale.
•collaboration among NGOs has been under-developed until recently. This is now improving somewhat, with national networks growing both on areas of common interest where capacity is limited (e.g. the Disability Law Network), and more broadly. This process still has a long way to go, as even within NGOs working on specific disabilities, coordination is often weak. With respect to disability-specific coordination, the experience of NGOs for the visually impaired offers an example of national coordination with positive results on policy. The other direction which shows promise in states such as Tamil Nadu and Orissa is state-specific disability networks which can mobilize the combined strengths of disability NGOs. The need for such coordination is imperative not only to realizing the full potential of the NGO movement, but also to minimizing uncoordinated initiatives which can undermine the coherence of the disability movement (e.g. researchers attribute the existence of four forms of sign language and around 12 different forms of Braille in India to earlier uncoordinated activities of NGOs in different parts of India).
•interactions with communities and PRIs: While rural penetration is in need of improvement in the NGO sector as it is in the public sector, the history of direct engagement with communities by disability NGOs – particularly through the CBR movement – suggests that they may also be a useful vehicle for engaging with GPs to raise awareness of disability issues. The example of Mamta Punarvas Kendra NGO in Shri Ganganagar district of Rajasthan provides an excellent case in point. The NGO has worked in one block to sensitize sarpanchs, GP members, patwaris and gram sevaks on disability issues, with field work for this report indicating that these efforts are already showing positive impact in implementation of poverty alleviation schemes. In addition, the NGO head has now become a panchayat samiti member.
•collaboration between NGOs and the private sector is growing, including in areas such supply of products to companies, training support and placement services. Experience in collaborations on training and employment is discussed in Chapter 5.
Overall, the disability NGO movement has contributed greatly to promoting the interests of PWD and awareness of their rights and situation. However, it remains in many ways an under-exploited resource in terms of fully mature partnerships between the public and NGO sectors. There are acknowledged shortcomings in the capacity of the disability NGO sector to grow into an expanded role, both in its own right and as a partner of government. These include lack of coordination within the NGO movement; need to include PWD themselves within NGOs and to partner more with DPOs; need to develop better internal systems for resource management and program M and E; need to broaden the skills base of NGOs from the traditional core of special educators and rehabilitation professionals to new skills such as legal advice, ITC-related training capacity, etc; need to increase penetration in rural areas, which will in turn demand new modes of service delivery for organizations often reliant on urban professionals as their personnel base. Despite these challenges, the disability NGO movement remains a critical actor in promoting full participation of PWD.
•Informal institutions and PWD: Previous research has confirmed that informal institutions – primarily the family – remain the most important factor in the lives of PWD. This section discusses briefly the role of informal institutions, focusing on the family and SHGs of PWD.
The failures of government, market and collective action in relation to disability reinforce the critical role of families in the lives of PWD. Other chapters provide evidence on the critical role of families – particularly the women in families – in providing support to PWD who require caring and other forms of support. For example, among the more than half of PWD in rural UP and TN who required at least some caring on a daily basis, this was provided by people outside the immediate household in less than 1 percent of cases. Such roles become increasingly important with ageing. The family also plays a major role in assisting the PWD to find employment, as results from the survey also indicate.
The family is not however an unambiguous source of support by any means for PWD. This can play out in several ways:
•the family may be over-protective of PWD members. This can be seen to some extent in the attitudes of parents of CWD to inclusive education reported in Chapter 4. It can also be seen in attitudes of parents in UP and TN towards employment of their PWD family member
•the family may – consciously or not – favour non-disabled household members over PWD (e.g. health evidence of this in child nutrition outcomes within households)
•the family may be a direct source of harm to the PWD member (as evidence from Orissa on physical and sexual abuse of PWD women reported in Chapter 2 suggests).
In some respects, the legal framework and customary law plays a role in the relative position of PWD within families. This has many dimensions. For example, both Hindu and Muslim traditions allow for dissolution of marriage in cases of mental instability of one partner. This is reflected in the 1955 Hindu marriage Act. There are also more specific examples like the prohibition on people with epilepsy and mental illness adopting children. In contrast, succession to property is not constrained under law by disability of any form.
Previous research and that for this report indicates quite clearly that there is a major awareness raising agenda on disability among family members of PWD. This can range from increasing knowledge on the causes and treatment of disability, entitlements under public schemes and availability of NGO and private services for PWD, exposure to success stories of PWD to raise awareness of the potential of PWD with the right opportunities, and other issues. While awareness campaigns often focus on the community, it seems even more critical as a first step to target families of PWD and PWD themselves (for whom self-esteem and other issues contribute to self-limitations in many cases).
The growth of the self-help movement also holds out significant potential for PWD. While experience with disability-specific SHGs is relatively limited in much of the country, certain states indicate the potential of PWD to mobilize and the potential for such mobilization to produce results. Karnataka is a case in point. Organizations such as Action for Disability and Development (ADD) India and Samuha have had sustained experience in promoting and building the capacity of PWD SHGs. In the case of Samuha, the SHGs are structured on a three tier level, with federations at taluk/district levels and a statewide network. Field work for this report reveals that these groups have improved accountability of district authorities in service delivery, as well as raising awareness among PWD of their rights, and issues related to detection, prevention of disabilities, and livelihoods. The experience of ADD in promoting formation of and strengthening PWD SHGs, and the achievements of those groups, is presented in Box 7.5. The Karnataka SHG experience is also linked to the relatively widespread penetration of Community-Based Rehabilitation (CBR) in the state (CBR is discussed in Chapter 3).
| Box 7.5: ADD India and the sangham approach to PWD SHGs | |
| ADD India has had a sustained program of support to SHGs of PWD in Karnataka and Tamil Nadu. As of 2004, it was estimated to have included around 20,000 people in its SHGs, a sharp increase from around 5,000 people in the mid-1990s. It has promoted SHG of PWD on a cross-disability basis, using a model of SHG with 7-20 members which meets twice monthly. Office bearing is rotated among the membership on the basis of elections. The SHGs (known as sanghams or associations) discuss the whole range of PWD issues in their village, and also take matters up with the local authorities. Many of them have a mutual savings system from which members can borrow either in emergencies or for income generation purposes. The sangham membes also participate in village development activities such as immunization drives. The PWD sanghams also link with womens’, youth and other groups to lobby on matters of mutual interest. The sanghams have also mobilized greater political participation among PWD. For example, in AP in the late 1990s, 31 PWD were elected to local panchayats (of a total of 78 standing), and members ensure regular representation in gram sabhas. In order to spread their expertise in facilitation and support to PWD SHGs, ADD have a training programme for NGO staff who wish to support similar efforts. The partnership with other NGOs is a key element of ADD’s model of promoting PWD SHGs. Source: UNESCAP (1997); ADD (UK) annual report, 2003-04. |
The challenge in SHGs is often to go to scale in terms of wide coverage. This may be an even bigger challenge for PWD SHGs, where capacity building needs may be greater in some cases. However, the experience of the AP Velugu programme (now IKP) indicates that wide coverage of PWD SHGs can be achieved within the context of major programs. As of late 2005, AP had over 130,000 people with disabilities formed into almost 15,000 SHGs which are in some areas federated at mandal and district levels. A similar initiative is also in progress in TN under a World Bank-financed community development project. While strengthening their capacity and moving to improved outcomes for PWD remains a challenge, the AP experience deserves close attention to assess the scope for a widescale PWD SHG movement.
Conclusions and recommendations
There are both policy and institutional reform needs in the disability sector. At this point, a focus on outcomes for people with disabilities would suggest that the priority should be on institutional reform and strengthening, reviewing the institutional framework in the disability sector and strengthening the capacity of institutions to deliver on policy commitments. Nonetheless, several broad policy reforms remain important. They include:
Policy Reforms. Disability policy reforms are needed in several areas: First, there should be serious consideration given to broadening the categories of disabled people included in the PWD Act, which may in any event be necessary in light of the new UN Convention to which India is a signatory. This may also require a de-linking of definitional inclusion of different groups with specific entitlements under the Act. While fiscal and other capacity issues suggest that not all disabled people may be supported through public interventions, this does not seem a good reason to exclude them from inclusion as PWD under the Act. Legislation and policy should ensure that clear obligations for involvement of persons with disabilities themselves at all stages of policy development, implementation and monitoring. Second, MSJE and central and state Commissioners’ offices should develop programs in collaboration with DPOs and NGOs for awareness raising of officials, service providers, PRI representatives and communities on programs for people with disabilities. A periodic monitoring of awareness, with particular focus on lagging states and remote regions, should be put in place to assess impact. States should be strongly encouraged to develop their own disability policies which elaborate a credible strategy for meeting their commitments under the PWD and other acts. The example of Chhattisgarh offers a useful example of such a policy. Finally, there should be a process for basic benchmarking of feasible policies and programs for people with disabilities in the areas which are currently subject to the economic capacity proviso.
Institutional reforms would seem desirable in several directions: First, the institutional framework at all levels needs to have a substantially strengthened direct role for persons with disabilities themselves. Second, responsibility for specific programs for PWD should be brought clearly under relevant line Ministries in some cases, e.g. bringing all education policies under MHRD as noted above. Third, GoI may like to consider overhauling the current coordinating mechanism into a National Commission for PWD, which would have the status and convening power which is currently under-developed in the sector. It is important that such a body be a coordination and oversight agency, and not be viewed as a separate “silo” for disability. Such an initiative would only make sense if the structural problems of coordination within and between levels of government, and between the public and non-governmental sectors are addressed. It would also require a transition strategy if the current Commissioners’ Offices are to be merged into a future Commission, so that there is not simply duplication of responsibilities. In this light, any move towards a Commission should not forestall the urgent need to strengthen the capacity of Commissioners’ Offices to perform their current functions, in particular on grievance redressal. Fourth, the enforcement mechanisms for the Act need to be clarified and strengthened. One option would be a Disability Tribunal with direct enforcement powers. This has pros and cons, as there is a risk of “over-judicializing” the grievance mechanisms for PWD and thus reducing their access. An alternative is obviously strengthening of both central and state Commissioners’ offices to play their grievance redressal function more effectively. A review of human resource and financial capacity of central and state Commissioners’ offices is also needed, and guidelines on minimum staffing levels introduced. The national policy and legislation needs to reflect the growing role of PRIs and use it as an opportunity to extend institutional reach to the village level, and more importantly to increase the local channels for accountability of public and other disability service providers. NGOs should also be brought more actively into both policy and implementation, but with strengthened financial accountability and monitoring of program outcomes. Finally, there needs to be more direct engagement between both public and NGO sectors with PWD themselves and their families, with SHGs being a logical vehicle.